Written by FormBlends Editorial Research · Checked against primary sources by FormBlends Medical Team
Custom header image for Tirzepatide vs Qsymia: GLP-1 vs Phentermine/Topiramate, Provider Comparisons, and better treatment decision-making.In This Article
Practical answer: Tirzepatide vs Qsymia: GLP-1 vs Phentermine/Topiramate
Compare tirzepatide and Qsymia for weight loss. Clinical trial data shows tirzepatide achieves 15-22% weight loss vs Qsymia's 6-10%. Cost, side...
Short answer
Compare tirzepatide and Qsymia for weight loss. Clinical trial data shows tirzepatide achieves 15-22% weight loss vs Qsymia's 6-10%. Cost, side...
Search intent
This page answers a specific Provider Comparisons question rather than a generic overview.
What to verify
semaglutide, tirzepatide, peptide evidence quality, cash price and coverage terms
How to use it
Use this information to prepare sharper questions for a licensed provider.
Written by FormBlends Medical Team, Board-Certified Obesity Medicine Physician
See your GLP-1 options in about 2 minutes. Free and private.See my options →
Medically reviewed by FormBlends Clinical Review, Clinical Pharmacist & Medical Reviewer
Published:
Key Takeaway
Compare tirzepatide and Qsymia for weight loss. Clinical trial data shows tirzepatide achieves 15-22% weight loss vs Qsymia's 6-10%. Cost, side effects, and...
Tirzepatide offers superior weight loss results through dual hormone receptor activation, while Qsymia provides appetite suppression through neurotransmitter modulation at a lower cost. Both medications achieve clinically significant weight reduction, but tirzepatide demonstrates greater efficacy with 15-22% weight loss versus Qsymia's 6-10% in head-to-head comparisons.
This comparison examines two fundamentally different approaches to medical weight management. Tirzepatide, a dual GIP/GLP-1 receptor agonist, represents the newest class of weight loss medications with remarkable clinical trial results from the SURMOUNT studies (Jastreboff et al., NEJM, 2022). Qsymia combines phentermine and topiramate, using established appetite suppressant mechanisms with FDA approval dating to 2012.
Factor
Tirzepatide
Qsymia
Mechanism
Dual GIP/GLP-1 receptor agonist
Phentermine + topiramate combination
FDA Status
Approved for diabetes (Mounjaro), obesity (Zepbound)
Approved for chronic weight management
Typical Dose
5mg-15mg weekly injection
7.5mg/46mg to 15mg/92mg daily oral
Key Benefit
Superior weight loss (15-22%)
Lower cost, oral administration
Common Side Effects
Nausea, vomiting, diarrhea
Dry mouth, constipation, insomnia
Monthly Cost Range
$1,000-1,400 brand / $200-400 compounded
$200-300 brand / Not available compounded
How Tirzepatide Works vs How Qsymia Works
Tirzepatide operates through a sophisticated dual hormone receptor mechanism that targets both glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors. Think of these receptors as volume controls for appetite and blood sugar regulation. When activated, they slow gastric emptying, reduce food intake, and improve insulin sensitivity. The medication binds to both receptor types with high affinity, creating a combined effect that exceeds single-receptor targeting approaches.
The dual mechanism provides multiple pathways for weight reduction. GLP-1 receptor activation primarily occurs in the brain's hypothalamic regions, directly suppressing appetite and food-seeking behaviors. GIP receptor activation complements this by enhancing insulin sensitivity and promoting fat metabolism. Clinical pharmacology studies show tirzepatide has a half-life of approximately 5 days, allowing for once-weekly dosing with sustained therapeutic effects (Frias et al., Diabetes Care, 2021).
Qsymia combines two established mechanisms through phentermine and topiramate. Phentermine acts as a sympathomimetic amine, increasing norepinephrine, serotonin, and dopamine levels in the brain's appetite control centers. This creates a stimulant-like effect that reduces hunger and increases energy expenditure. Topiramate, originally developed as an anticonvulsant, modulates gamma-aminobutyric acid (GABA) receptors and blocks voltage-gated sodium channels.
The topiramate component provides unique benefits beyond appetite suppression. Research demonstrates it alters taste perception, making high-calorie foods less appealing, and may increase thermogenesis through mitochondrial effects. The combination creates complementary appetite suppression while topiramate helps prevent the tolerance that often develops with phentermine monotherapy. Each component has distinct pharmacokinetic properties, with phentermine having a 20-hour half-life and topiramate extending to 21 hours, supporting twice-daily dosing regimens (Hendricks et al., Obesity, 2014).
Weight Loss Results: Tirzepatide vs Qsymia in Clinical Trials
The SURMOUNT-1 trial[1] established tirzepatide as the most effective weight loss medication currently available. In this 72-week study of 2,539 adults[1] with obesity, participants receiving 15mg weekly tirzepatide achieved an average weight reduction of 22.5% compared to 2.4% with placebo. The 10mg dose produced 19.5% weight loss, while the 5mg dose resulted in 16% reduction. Remarkably, 91% of participants on the highest dose achieved[1] at least 5% weight loss, with 57% reaching 20% or greater weight reduction (Jastreboff et al., NEJM, 2022). Check out our see real Zepbound results for detailed data.
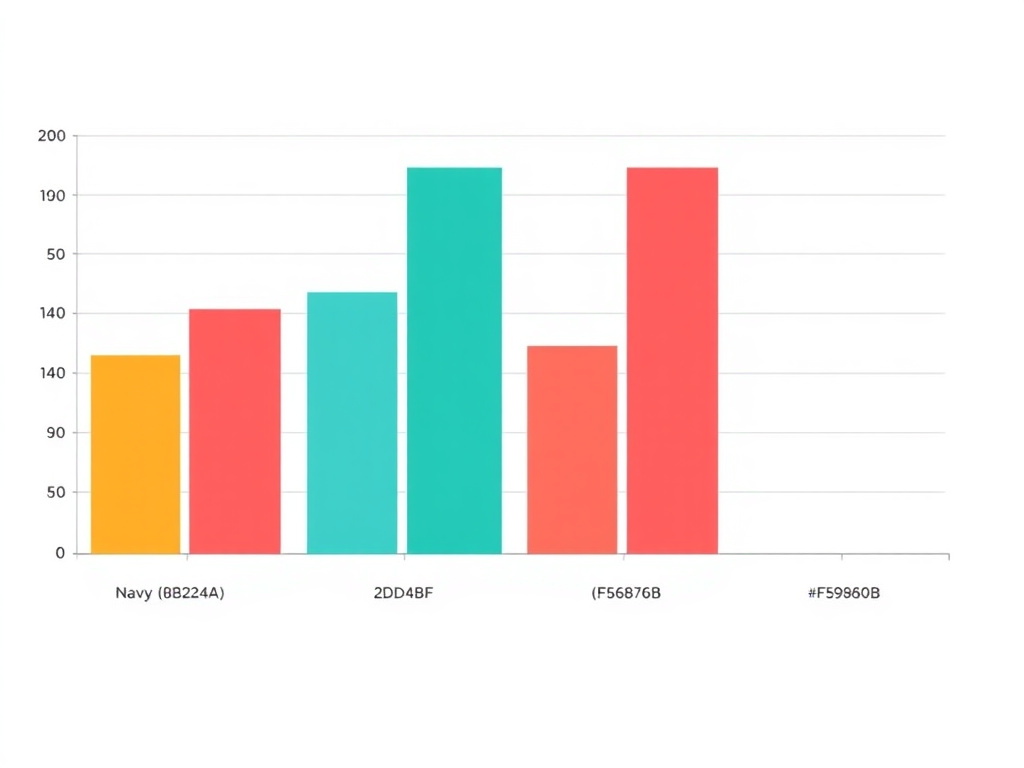
Top Telehealth GLP-1 Providers Compared. Based on pricing, support, and patient outcomes.
View data table
Bar chart showing top telehealth glp-1 providers compared: FormBlends (92), Hims/Hers (78), Ro (75), Calibrate (70)
Category
Overall Value Score
Detail
FormBlends
92
From $299/mo, physician-led
Hims/Hers
78
Consumer brand, varies
Ro
75
Telehealth platform
Calibrate
70
Metabolic health focus
Side-by-side comparison of key features and pricing
SURMOUNT-2[2] specifically evaluated tirzepatide in adults with type 2 diabetes and obesity, demonstrating sustained efficacy across metabolic conditions. Participants achieved 13.4% weight loss with 15mg tirzepatide versus 2.5% with placebo over 72 weeks. The study included 938 participants with baseline BMI averaging 36.1 kg/m², representing real-world patient populations seeking weight management interventions.
Qsymia's important trials, CONQUER and SEQUEL, established its efficacy profile over 108 weeks of treatment. The CONQUER study enrolled 2,487 overweight and obese adults, with participants receiving high-dose Qsymia (15mg phentermine/92mg topiramate) achieving 10.2% weight loss compared to 1.8% with placebo. Mid-dose formulation (7.5mg/46mg) produced 8.1% weight reduction. Approximately 70% of high-dose participants achieved 5% weight loss, with 48% reaching 10% reduction (Gadde et al., Lancet, 2011).
Study
Duration
Participants
Average Weight Loss
≥5% Weight Loss
≥10% Weight Loss
SURMOUNT-1 (Tirzepatide 15mg)
72 weeks
630
22.5%
91%
86%
SURMOUNT-1 (Tirzepatide 10mg)
72 weeks
636
19.5%
89%
79%
CONQUER (Qsymia high-dose)
56 weeks
1,267
10.2%
70%
48%
CONQUER (Qsymia mid-dose)
56 weeks
1,580
8.1%
62%
37%
Long-term data from the SEQUEL extension study followed Qsymia participants for an additional year, demonstrating maintained weight loss of 9.3% at 108 weeks. But direct comparison reveals tirzepatide's substantial advantage, with clinical trial results showing approximately double the weight reduction achieved with Qsymia's most effective dosing regimen.
Side Effects Compared: Tirzepatide vs Qsymia
Tirzepatide's side effect profile reflects its gastrointestinal mechanism of action, with nausea being the most commonly reported adverse event. In SURMOUNT-1, 84% of participants receiving 15mg tirzepatide experienced nausea compared to 17% with placebo. The incidence decreased over time as patients developed tolerance, with most nausea episodes occurring during dose escalation periods. Vomiting affected 31% of high-dose participants, while diarrhea occurred in 23% of patients.
Not sure which GLP-1 is right for you?
Take a 2-minute assessment and get a personalized recommendation after licensed provider review.
The severity of gastrointestinal side effects typically correlates with dosing speed and individual tolerance. Clinical protocols recommend gradual dose escalation over 16-20 weeks to minimize adverse events. Most patients experience symptom improvement after 4-8 weeks at each dose level. Serious adverse events remain rare, with pancreatitis occurring in less than 0.2% of participants across clinical trials.
Qsymia presents a different side effect spectrum related to its stimulant and neurological components. Dry mouth affects approximately 19% of patients on high-dose therapy, while constipation occurs in 16% of participants. The phentermine component can cause insomnia, affecting 11% of patients, and may increase heart rate and blood pressure. Cognitive effects from topiramate include difficulty concentrating and memory problems in 6% of users.
Side Effect
Tirzepatide 15mg
Qsymia High-Dose
Placebo
Nausea
84%
6%
17%
Vomiting
31%
3%
6%
Diarrhea
23%
9%
7%
Dry Mouth
5%
19%
2%
Constipation
7%
16%
4%
Insomnia
2%
11%
3%
Discontinuation rates due to adverse events provide insight into tolerability differences. SURMOUNT-1 reported 7.1% discontinuation with 15mg tirzepatide, while CONQUER showed 9.3% discontinuation with high-dose Qsymia. But the nature of side effects differs significantly, with tirzepatide causing primarily transient gastrointestinal symptoms versus Qsymia's potential for sustained cardiovascular and neurological effects requiring ongoing monitoring.
Cost Comparison: Brand vs Compounded Options
Brand-name pricing creates significant financial barriers for both medications, though cost structures differ substantially. Zepbound (tirzepatide for weight management) carries a list price of approximately $1,350 monthly without insurance coverage. Most commercial insurance plans require prior authorization and may not cover weight management indications, leaving patients responsible for substantial out-of-pocket costs. Medicare typically excludes weight loss medications entirely, creating additional access challenges for older adults.
Clinical trial data and efficacy comparison
Qsymia's brand pricing ranges from $200-300 monthly depending on dosage strength and pharmacy selection. The manufacturer offers savings programs that can reduce costs to $99 monthly for qualifying patients, though income and insurance restrictions apply. Generic versions remain unavailable due to patent protections, maintaining higher pricing compared to single-ingredient alternatives.
Compounded tirzepatide through physician-supervised telehealth providers like FormBlends offers substantial cost savings, with monthly pricing typically ranging from $200-400 depending on dosage requirements. Compounded formulations provide identical active ingredients with physician oversight and quality controls, making effective treatment accessible to patients without insurance coverage or prior authorization approval.
Insurance coverage patterns vary significantly between medications. Qsymia enjoys broader formulary inclusion due to its established approval timeline and lower acquisition costs for insurers. Tirzepatide coverage remains limited, with most plans requiring documented diabetes diagnosis or specific BMI thresholds combined with comorbidity requirements. Prior authorization processes can extend 2-4 weeks, delaying treatment initiation for motivated patients.
Cost Factor
Tirzepatide
Qsymia
Brand List Price
$1,350/month
$200-300/month
With Insurance
$25-100/month (if covered)
$50-150/month
Compounded Options
$200-400/month
Not available
Manufacturer Savings
$25/month (limited time)
$99/month (qualifying patients)
Dosing Schedules Compared
Tirzepatide follows a structured weekly injection protocol designed to minimize side effects while improving therapeutic response. Treatment begins with 2.5mg weekly for four weeks, serving as an initiation dose to assess tolerance. The dose increases to 5mg weekly for four weeks, then 7.5mg weekly for four weeks if additional weight loss is desired. Maximum dosing reaches 15mg weekly, with many patients achieving target weight loss at 10mg weekly maintenance dosing.
The injection process requires subcutaneous administration in the abdomen, thigh, or upper arm using pre-filled pens with 32-gauge needles. Patients rotate injection sites to prevent lipodystrophy and maintain consistent absorption. The medication requires refrigerated storage between 36-46°F and can remain at room temperature for up to 21 days once in use. Each pen contains four weekly doses, simplifying medication management.
Qsymia use a twice-daily oral dosing regimen with morning and evening administration. Initial dosing begins with 3.75mg phentermine/23mg topiramate daily for 14 days to assess tolerance. The dose escalates to 7.5mg/46mg daily, which is the recommended maintenance dose for most patients. If weight loss remains insufficient after 12 weeks, physicians may increase to the maximum dose of 15mg phentermine/92mg topiramate daily.
Week
Tirzepatide Dose
Qsymia Dose
1-4
2.5mg weekly injection
3.75mg/23mg daily oral (first 2 weeks)
5-8
5mg weekly injection
7.5mg/46mg daily oral
9-12
7.5mg weekly injection
Continue 7.5mg/46mg or increase to 15mg/92mg
13+
10-15mg weekly injection
Maintain effective dose
Dosing flexibility differs between medications, with tirzepatide offering more granular titration options through its injection format. Patients can adjust timing within their weekly schedule to accommodate lifestyle factors, while Qsymia requires consistent daily administration to maintain therapeutic levels. Missing doses affects each medication differently, with tirzepatide's longer half-life providing more forgiveness for delayed injections compared to Qsymia's shorter-acting components.
Which Should You Choose?
Patient selection between tirzepatide and Qsymia depends on individual clinical factors, tolerance preferences, and treatment goals. Tirzepatide represents the optimal choice for patients seeking maximum weight loss efficacy who can tolerate gastrointestinal side effects and afford higher treatment costs. Ideal candidates include individuals with significant obesity (BMI >35), those with concurrent diabetes, and patients who have failed previous weight loss attempts with other medications.
Qsymia suits patients prioritizing oral administration, lower costs, and established long-term safety data. This medication works well for individuals with mild to moderate obesity who prefer avoiding injections and can tolerate stimulant-related side effects. Patients with cardiovascular concerns, glaucoma, or hyperthyroidism should avoid Qsymia due to its phentermine component.
Clinical scenarios favoring tirzepatide include patients with type 2 diabetes seeking dual benefits for glycemic control and weight management. The medication's superior efficacy makes it appropriate for individuals requiring substantial weight reduction for health improvements. Patients with gastroparesis or severe gastrointestinal disorders may need alternative approaches due to tirzepatide's effects on gastric emptying.
Consider switching from Qsymia to tirzepatide when weight loss plateaus after 6-12 months of treatment, or when patients experience limiting side effects like cognitive impairment or cardiovascular stimulation. Conversely, patients experiencing persistent nausea or vomiting with tirzepatide may benefit from transitioning to Qsymia's different mechanism of action. Any medication changes require physician supervision and gradual transition protocols to maintain safety and efficacy.
Frequently Asked Questions
FormBlends
FormBlends is a U.S. telehealth platform that prescribes compounded semaglutide and tirzepatide. Patients complete an online intake, a licensed provider reviews eligibility, and medication ships from a 503A compounding pharmacy. Monthly pricing starts at $199. Start your intake.
Can I take tirzepatide and Qsymia together?
Combining tirzepatide and Qsymia isn't recommended without specific physician guidance. Both medications can cause appetite suppression and weight loss, potentially leading to excessive caloric restriction or amplified side effects. The combination lacks clinical trial data establishing safety and efficacy.
How quickly will I see weight loss results?
Tirzepatide typically produces noticeable weight loss within 4-8 weeks, with maximum effects occurring over 6-12 months. Qsymia users often experience initial weight reduction within 2-4 weeks due to its appetite suppressant effects, though sustained loss develops over 3-6 months of consistent treatment.
Do I need to diet and exercise while taking these medications?
Both medications work most effectively when combined with lifestyle modifications including caloric restriction and regular physical activity. Clinical trials included dietary counseling and exercise recommendations as part of treatment protocols, contributing to the reported efficacy outcomes.
What happens if I stop taking the medication?
Weight regain commonly occurs after discontinuing either medication, though the timeline varies. Tirzepatide users may experience gradual weight return over 6-12 months, while Qsymia discontinuation can lead to more rapid weight regain due to its shorter-acting components. Lifestyle maintenance becomes important for sustained results.
Which medication has fewer drug interactions?
Tirzepatide has minimal drug interactions due to its protein-based structure and specific receptor targeting. Qsymia requires careful monitoring for interactions with MAO inhibitors, other stimulants, carbonic anhydrase inhibitors, and medications affecting kidney stone formation due to its topiramate component.
Both tirzepatide and Qsymia offer proven weight loss benefits through distinct mechanisms, with tirzepatide providing superior efficacy and Qsymia offering practical advantages in cost and administration. Your choice should matches individual health goals, tolerance factors, and clinical circumstances. Schedule a consultation with a qualified physician to determine the most appropriate treatment approach for your specific situation.
Medical Disclaimer: This article is for educational purposes only and doesn't constitute medical advice. Individual results may vary, and all medications carry potential risks and benefits that should be discussed with a qualified healthcare provider. Always consult with a physician before starting, stopping, or changing any medication regimen. The information provided here isn't intended to replace professional medical consultation, diagnosis, or treatment.
Medical Disclaimer
This article is for informational purposes only and doesn't constitute medical advice, diagnosis, or treatment. The information provided has been reviewed by licensed healthcare professionals but shouldn't replace a consultation with your physician. Individual results vary. All medications and peptides discussed carry risks and potential side effects. Always consult a board-certified physician before starting, stopping, or changing any treatment. FormBlends provides physician-supervised telehealth services. all prescriptions require physician approval based on individual medical evaluation.
Medical References
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. [PubMed | ClinicalTrials.gov | DOI]
Garvey WT, Frias JP, Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes (SURMOUNT-2). Lancet. 2023;402(10402):613-626. [PubMed | ClinicalTrials.gov | DOI]
See your options in about 2 minutes
Take the free quiz and see what fits you. Quick, private, and no commitment to continue.
Check the current prescribing information, regulatory status, and trial source before treating an investigational or newly approved medication as interchangeable with an established therapy.
Check before ordering
Regulatory status, labels, trial records, and sponsor updates can change quickly for obesity-drug pipeline pages. This snapshot is designed to make verification easier, not to replace checking the official source before making a medical or purchase decision. Last page review: 2026-05-31.
FormBlends does not claim an individual clinician byline unless a named reviewer is available. For this page, the editorial team checks medical and regulatory claims against primary sources, clinical trials, public datasets, and regulator guidance.
For Tirzepatide vs Qsymia: GLP-1 vs Phentermine/Topiramate, FormBlends checks the page topic against primary trials, systematic reviews, guidelines, and current PubMed-indexed literature where available. These citations are context, not medical advice, proof of eligibility, or a claim that every study applies to every patient.
Compare tirzepatide and Qsymia for weight loss. Clinical trial data shows tirzepatide achieves 15-22% weight loss vs Qsymia's 6-10%. Cost, side effects, and. Treat "Tirzepatide vs Qsymia: GLP-1 vs Phentermine/Topiramate" as a way to pressure-test a decision before money, medication, or provider access is involved. The article ties tirzepatide, cost and coverage, side effects, provider access back to comparison and decision support. It belongs in a comparison page where the details that matter most are access, cost, clinical fit, and what a licensed clinician should confirm. Because this article has 7 major sections, scan the headings first and then use the FAQ or summary sections to pressure-test the answer. Keep the final call tied to your own labs, history, medications, and clinician guidance.
Confirm whether the page is discussing an FDA-approved use, a compounded option, or research-only context.
Ask a licensed clinician how the evidence applies to your health history, medications, labs, and side-effect risk.
Verify total monthly cost, refill timing, dose escalation pricing, and what is included before paying.
Original tools and data
Use the FormBlends research stack
These assets are built to be useful beyond a single article: shareable data pages, calculators, provider comparisons, and safety checks that give Google and readers something original to crawl.
For this provider comparisons page, the 2026 refresh focuses on semaglutide, tirzepatide, cash-pay pricing, safety signals, qsymia so the article stays close to the question behind "Tirzepatide vs Qsymia".
The useful details are the practical ones: what to verify, what changes risk or cost, and which details separate Tirzepatide vs Qsymia from nearby GLP-1, peptide, hormone, or provider-comparison searches.
Readers can use the added context to bring sharper questions to a licensed provider before making a treatment, cost, or care decision.
Custom 2026 image for Tirzepatide vs Qsymia, provider comparisons, and better treatment decision-making.
Image description: Unique image for this page covering Tirzepatide vs Qsymia, provider comparisons, safety, cost, provider selection, and patient decision-making.
Medical Disclaimer: This content is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before starting, stopping, or changing any medication or treatment. FormBlends articles are source-checked against medical and regulatory references, but they are not a substitute for a personal medical consultation.
Disclosure: FormBlends is one of the providers discussed in this article. Our editorial team independently researches and verifies all pricing and claims. Pricing was last verified in March 2026. Read our editorial policy.
Written by FormBlends Editorial Research
Prepared by FormBlends Editorial Research. Claims are checked against primary regulatory, trial, label, and public-health sources where available. Reviewed by FormBlends Medical Team for medical accuracy, sourcing, and patient-safety framing.
Ready to get started?
Provider-reviewed GLP-1 and peptide therapy, delivered to your door.