Executive Summary

Key Takeaways
- GLP-1 receptor agonists reduce three-point MACE (cardiovascular death, non-fatal MI, non-fatal stroke) by 12-26% across major CVOTs.
- The SELECT trial demonstrated a 20% MACE reduction in non-diabetic obese patients with atherosclerotic CVD, the first such evidence for this population.
- Cardiovascular benefits appear to be partly independent of weight loss, involving direct anti-inflammatory, anti-atherosclerotic, and vasculoprotective mechanisms.
- Heart failure outcomes data from STEP-HFpEF and SUMMIT show clinically meaningful improvements in symptoms, function, and hard endpoints.
- Guidelines now recommend GLP-1 RAs with proven CV benefit as first-line therapy in T2D patients with or at high risk for ASCVD, regardless of glycemic status.
GLP-1 receptor agonists are no longer just diabetes drugs. They are now among the most evidence-backed pharmacological tools for reducing major adverse cardiovascular events, including heart attack, stroke, and cardiovascular death. Multiple large-scale cardiovascular outcomes trials, enrolling over 60,000 patients collectively, have demonstrated consistent reductions in three-point MACE ranging from 12% to 26%.
The story of semaglutide and cardiovascular protection began with regulatory mandates. After safety concerns surrounding older diabetes medications in the early 2000s, the FDA required all new glucose-lowering drugs to undergo rigorous cardiovascular outcomes trials (CVOTs). What was initially a safety check turned into one of the most significant therapeutic discoveries of the last two decades. GLP-1 receptor agonists didn't just prove safe for the heart. They proved protective.
The LEADER trial in 2016 was the first to demonstrate that liraglutide significantly reduced three-point MACE by 13% compared to placebo in patients with type 2 diabetes and high cardiovascular risk. SUSTAIN-6 followed shortly after, showing that subcutaneous semaglutide lowered MACE by 26%, driven primarily by a striking 39% reduction in non-fatal stroke. The REWIND trial expanded the evidence base by including a broader population with lower baseline cardiovascular risk, and dulaglutide still achieved a 12% MACE reduction. These results weren't flukes. They were consistent signals from well-powered, placebo-controlled trials conducted across dozens of countries.
Then came SELECT. Published in 2023, the SELECT trial was a watershed moment. For the first time, a GLP-1 receptor agonist was tested specifically for cardiovascular risk reduction in patients who were overweight or obese but did not have diabetes. The trial enrolled 17,604 adults aged 45 and older with established atherosclerotic cardiovascular disease and a BMI of 27 or higher. Semaglutide 2.4 mg weekly reduced three-point MACE by 20% over a median follow-up of 39.8 months. This finding shattered the assumption that GLP-1 cardiovascular benefits were limited to the diabetic population and opened the door to a much wider clinical application.
What makes these cardiovascular benefits so compelling is that they appear to go beyond what weight loss alone can explain. Mediation analyses from SELECT suggest that only about 40% of the MACE reduction can be attributed to changes in body weight. The remaining benefit likely stems from direct anti-inflammatory effects, improvements in endothelial function, reductions in oxidative stress, favorable changes in lipid profiles, and direct actions on GLP-1 receptors expressed in heart tissue and blood vessels. C-reactive protein levels, a marker of systemic inflammation, dropped by approximately 40% in SELECT participants receiving semaglutide.
The heart failure data add another dimension to the cardiovascular story. The STEP-HFpEF trial demonstrated that semaglutide 2.4 mg improved symptoms, physical limitations, and exercise function in patients with obesity-related heart failure with preserved ejection fraction (HFpEF). Kansas City Cardiomyopathy Questionnaire scores improved by 7.8 points more than placebo at 52 weeks, a clinically meaningful difference. And tirzepatide, the dual GIP/GLP-1 receptor agonist, showed even larger improvements in the SUMMIT trial, reducing a composite of cardiovascular death and worsening heart failure events by 38%.
Blood pressure reductions of 3-6 mmHg systolic, modest improvements in triglycerides and LDL cholesterol, and reductions in visceral adiposity all contribute to the overall cardiovascular risk profile improvement. These metabolic effects begin early, often within the first few weeks of treatment, and persist throughout therapy.
Clinical guidelines have rapidly evolved to reflect this evidence. The 2023 AHA/ACC/ADA guidelines now recommend GLP-1 receptor agonists with proven cardiovascular benefit as first-line therapy for patients with type 2 diabetes and established or high-risk atherosclerotic cardiovascular disease, independent of HbA1c levels. The SELECT data are pushing these recommendations even further, with discussions underway about extending GLP-1 prescribing to non-diabetic patients with obesity and cardiovascular disease.
This report examines the full scope of cardiovascular evidence for GLP-1 receptor agonists. We'll cover the biological mechanisms through which these agents protect the heart, the clinical trial data that established their efficacy, the emerging heart failure evidence, the weight-independent pathways of cardioprotection, and the practical implications for clinical decision-making. For a broader understanding of the GLP-1 class, see our GLP-1 class overview.
Key Takeaways
- GLP-1 receptor agonists reduce three-point MACE (cardiovascular death, non-fatal MI, non-fatal stroke) by 12-26% across major CVOTs.
- The SELECT trial demonstrated a 20% MACE reduction in non-diabetic obese patients with atherosclerotic CVD, the first such evidence for this population.
- Cardiovascular benefits appear to be partly independent of weight loss, involving direct anti-inflammatory, anti-atherosclerotic, and vasculoprotective mechanisms.
- Heart failure outcomes data from STEP-HFpEF and SUMMIT show clinically meaningful improvements in symptoms, function, and hard endpoints.
- Guidelines now recommend GLP-1 RAs with proven CV benefit as first-line therapy in T2D patients with or at high risk for ASCVD, regardless of glycemic status.
GLP-1 Receptors in the Cardiovascular System

Figure 2: GLP-1 receptors are expressed across multiple cardiovascular tissue types, including cardiomyocytes, endothelial cells, and vascular smooth muscle, providing a biological basis for the direct cardiac effects observed in clinical trials.
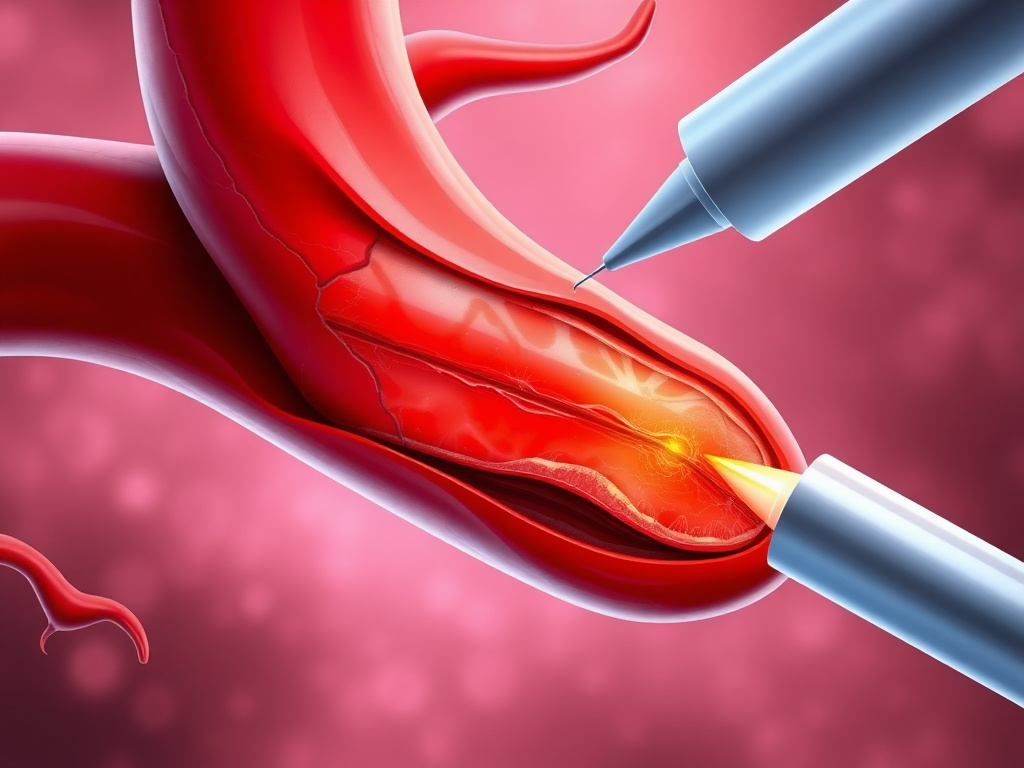
The cardiovascular effects of GLP-1 receptor agonists aren't simply downstream consequences of improved metabolism. GLP-1 receptors are expressed directly in heart and vascular tissue, creating a biological foundation for the cardioprotective effects observed in large-scale clinical trials. Understanding this receptor distribution helps explain why these agents do more for the heart than weight loss or glucose control alone would predict.
Discovery and Distribution of Cardiovascular GLP-1 Receptors
The GLP-1 receptor (GLP-1R) is a class B G-protein-coupled receptor that was first characterized in pancreatic beta cells, where it mediates glucose-dependent insulin secretion. But research over the past two decades has revealed that GLP-1R expression extends far beyond the pancreas. In the cardiovascular system, GLP-1 receptors have been identified in cardiomyocytes, the sinoatrial node, vascular endothelial cells, vascular smooth muscle cells, and cardiac fibroblasts. This widespread expression pattern was first mapped in detail using receptor autoradiography and later confirmed through RT-PCR, immunohistochemistry, and reporter gene studies in both animal models and human tissue samples.
In human hearts, GLP-1R mRNA is expressed at particularly high levels in the atria, with lower but detectable expression in the ventricles. The sinoatrial node shows significant receptor density, which explains the modest heart rate increase (2-4 beats per minute) consistently observed with GLP-1 receptor agonist therapy. This heart rate effect is a direct pharmacological consequence of receptor activation in the cardiac conduction system, not a reflex response to vasodilation or other hemodynamic changes.
Murine studies using GLP-1R knockout mice have provided critical evidence for the functional significance of these cardiac receptors. GLP-1R-deficient mice develop increased left ventricular wall thickness, impaired left ventricular contractility, and diastolic dysfunction even at young ages. These structural and functional abnormalities suggest that basal GLP-1 receptor signaling plays a tonic role in maintaining normal cardiac structure and function, independent of any pharmacological intervention.
Receptor Signaling in Cardiomyocytes
When a GLP-1 receptor agonist binds to GLP-1R on cardiomyocytes, it activates the canonical Gs-adenylyl cyclase-cAMP-PKA signaling cascade. This pathway has several downstream effects relevant to cardiac protection. First, cAMP-dependent signaling enhances myocardial glucose uptake through translocation of GLUT1 and GLUT4 transporters to the cell membrane. This is especially significant during ischemic conditions when the heart's usual preference for fatty acid oxidation becomes maladaptive, and a metabolic shift toward glucose utilization improves energy efficiency and reduces oxygen consumption.
PKA activation also phosphorylates several targets involved in calcium handling, including phospholamban and the ryanodine receptor (RyR2). The net effect is improved sarcoplasmic reticulum calcium cycling, which can enhance contractile function without the arrhythmogenic risk associated with higher intracellular calcium loads. Preclinical studies have shown that liraglutide improves calcium transients in isolated cardiomyocytes from failing hearts, suggesting a direct inotropic benefit mediated through receptor signaling.
Beyond the cAMP-PKA pathway, GLP-1 receptor activation in cardiomyocytes engages several pro-survival signaling cascades. The PI3K-Akt pathway is activated downstream of GLP-1R, leading to phosphorylation and inactivation of pro-apoptotic proteins including BAD, caspase-9, and glycogen synthase kinase-3 beta (GSK-3β). This anti-apoptotic signaling is particularly relevant during ischemia-reperfusion injury, where cardiomyocyte death drives infarct expansion and adverse remodeling. Studies in rat models of myocardial infarction have shown that pre-treatment with GLP-1 receptor agonists reduces infarct size by 30-50% when administered before coronary artery occlusion.
Activation of AMPK (AMP-activated protein kinase) is another downstream consequence of GLP-1R signaling in the heart. AMPK serves as a cellular energy sensor and, when activated, promotes metabolic pathways that generate ATP while suppressing energy-consuming processes. In the context of myocardial ischemia, AMPK activation enhances fatty acid oxidation during the reperfusion phase, stimulates mitochondrial biogenesis, and reduces endoplasmic reticulum stress. These effects collectively improve the heart's ability to recover from ischemic insults.
Effects on Vascular Endothelium
Endothelial cells line every blood vessel in the body and play a central role in vascular homeostasis, regulating tone, permeability, coagulation, and inflammation. GLP-1 receptors on endothelial cells mediate several protective effects that are directly relevant to atherosclerosis and cardiovascular risk. When semaglutide or other GLP-1 RAs bind to endothelial GLP-1 receptors, they stimulate nitric oxide (NO) production through activation of endothelial nitric oxide synthase (eNOS). This occurs via both the cAMP-PKA pathway and the PI3K-Akt-eNOS cascade. Increased NO bioavailability leads to vasodilation, reduced platelet aggregation, and decreased leukocyte adhesion to the vessel wall.
Flow-mediated dilation (FMD), a non-invasive measure of endothelial function, improves with GLP-1 receptor agonist therapy. A meta-analysis of 12 clinical studies found that GLP-1 RAs improved FMD by an average of 1.8% compared to control treatments, an effect size comparable to that of statins. This improvement in endothelial function occurs within weeks of initiating therapy and persists throughout treatment, suggesting a sustained pharmacological effect rather than a transient response.
GLP-1 receptor activation also reduces endothelial expression of adhesion molecules, including VCAM-1, ICAM-1, and E-selectin. These molecules are upregulated by inflammatory cytokines and oxidized LDL, and they serve as docking sites for circulating monocytes during the initiation of atherosclerosis. By reducing adhesion molecule expression, GLP-1 RAs directly inhibit one of the earliest steps in atherogenesis. In vitro studies using human umbilical vein endothelial cells (HUVECs) exposed to TNF-alpha showed that liraglutide reduced VCAM-1 expression by approximately 40% and monocyte adhesion by 35%, effects that were abolished by GLP-1R antagonism with exendin 9-39.
Endothelial permeability is another target. GLP-1 receptor signaling strengthens endothelial barrier function by promoting the assembly of tight junction proteins including ZO-1 and occludin. This is particularly relevant in the context of diabetic vasculopathy, where hyperglycemia-induced endothelial barrier breakdown contributes to vascular leakage and edema. But the barrier-protective effects of GLP-1 RAs extend beyond the diabetic context, as demonstrated in the SELECT trial population of non-diabetic patients.
Vascular Smooth Muscle Effects
Vascular smooth muscle cells (VSMCs) are the contractile cells of the arterial wall, and their behavior is central to both blood pressure regulation and atherosclerotic plaque development. GLP-1 receptors on VSMCs mediate relaxation through cAMP-dependent inhibition of myosin light chain kinase, contributing to the blood pressure-lowering effect of GLP-1 RAs. This direct vascular relaxation is independent of endothelium-derived NO and represents an additional mechanism of vasodilation.
Perhaps more significant is the effect of GLP-1R activation on VSMC phenotype switching. In atherosclerosis, VSMCs undergo a transition from a contractile, quiescent phenotype to a synthetic, proliferative phenotype that contributes to neointimal formation and plaque growth. GLP-1 receptor agonists have been shown to inhibit this phenotypic switch in preclinical models. Liraglutide reduced VSMC proliferation by 25-30% in ex vivo studies using human coronary artery smooth muscle cells stimulated with platelet-derived growth factor (PDGF). The mechanism involves cAMP-mediated inhibition of the ERK1/2 pathway, which is a key driver of VSMC proliferation.
VSMCs also contribute to arterial calcification, a process that stiffens blood vessels and independently predicts cardiovascular events. Preliminary evidence suggests that GLP-1R signaling may attenuate VSMC calcification by suppressing osteogenic transcription factors including Runx2 and alkaline phosphatase. While this area requires more clinical validation, it represents a potentially significant mechanism of vascular protection, particularly in the aging population where arterial calcification is highly prevalent.
Cardiac Fibroblasts and Remodeling
Cardiac fibroblasts are the most abundant non-myocyte cell type in the heart and play a central role in extracellular matrix homeostasis and wound repair. Following myocardial injury, fibroblasts become activated, proliferate, and differentiate into myofibroblasts that produce excessive collagen, leading to fibrosis. Cardiac fibrosis impairs both systolic and diastolic function and is a key driver of heart failure progression.
GLP-1 receptors on cardiac fibroblasts mediate anti-fibrotic effects through suppression of transforming growth factor-beta (TGF-β) signaling. In rodent models of pressure-overload heart failure, treatment with GLP-1 RAs reduced myocardial collagen content by 20-40% and attenuated the expression of pro-fibrotic genes including collagen I, collagen III, and fibronectin. The cAMP-Epac-Rap1 signaling axis appears to be the primary mediator, as Epac-selective cAMP analogs replicate the anti-fibrotic effects of GLP-1R activation.
Matrix metalloproteinases (MMPs), the enzymes responsible for extracellular matrix degradation, are also modulated by GLP-1R signaling. Liraglutide has been shown to reduce MMP-2 and MMP-9 activity in cardiac tissue from mice subjected to myocardial infarction, an effect associated with reduced ventricular dilation and improved post-infarct remodeling. These findings are consistent with the observation that GLP-1 RA-treated patients show less adverse cardiac remodeling on serial echocardiographic studies.
Autonomic and Neural Cardiovascular Effects
GLP-1 receptors in the brainstem, particularly in the nucleus of the solitary tract and the area postrema, influence cardiovascular regulation through modulation of autonomic outflow. Activation of these central GLP-1 receptors increases sympathetic tone to the heart, which explains the modest (2-4 bpm) increase in heart rate consistently observed with GLP-1 RA therapy. This effect is mediated through reduced vagal tone rather than direct sympathetic activation, as demonstrated by heart rate variability analyses showing decreased high-frequency power (a marker of parasympathetic activity).
Despite concerns that sustained heart rate elevation might be harmful, the clinical evidence consistently shows net cardiovascular benefit with GLP-1 RAs. The modest chronotropic effect does not appear to offset the substantial benefits derived from anti-inflammatory, anti-atherosclerotic, and direct cardioprotective mechanisms. In LEADER, the cardiovascular benefit of liraglutide was maintained even in subgroup analyses that accounted for heart rate changes, and in SELECT, the 20% MACE reduction occurred despite a mean heart rate increase of approximately 3 bpm.
Central GLP-1R activation also modulates blood pressure through effects on renal sympathetic nerve activity and the renin-angiotensin-aldosterone system (RAAS). GLP-1 RAs promote natriuresis through direct effects on renal tubular sodium handling and through suppression of angiotensin II levels. These renal and neurohumoral effects contribute to the 3-6 mmHg reduction in systolic blood pressure observed across clinical trials, an effect that is additive to the weight loss-mediated blood pressure reduction. For more on GLP-1 mechanisms of action, see our weight loss mechanisms guide.
Clinical Significance
The expression of GLP-1 receptors across cardiomyocytes, endothelial cells, vascular smooth muscle, and cardiac fibroblasts provides the mechanistic framework for understanding why cardiovascular benefits of GLP-1 RAs go beyond metabolic improvements. Direct receptor-mediated effects on cell survival, inflammation, fibrosis, and vascular function operate in parallel with the indirect benefits of weight loss and glycemic control, explaining the "weight-independent" cardioprotection observed in mediation analyses from SELECT and other CVOTs.
Anti-Inflammatory & Anti-Atherosclerotic Effects
Atherosclerosis is fundamentally an inflammatory disease. The progression from fatty streak to vulnerable plaque is driven by chronic low-grade inflammation involving macrophages, T cells, smooth muscle cells, and a cascade of cytokines. GLP-1 receptor agonists intervene at multiple points in this inflammatory pathway, reducing systemic inflammation markers, modulating immune cell behavior, stabilizing existing plaques, and restoring endothelial barrier integrity.
Systemic Inflammation: CRP and Beyond
High-sensitivity C-reactive protein (hsCRP) is the most widely studied biomarker of systemic inflammation and an independent predictor of cardiovascular events. Across GLP-1 receptor agonist trials, consistent and substantial reductions in hsCRP have been observed. In the SELECT trial, semaglutide 2.4 mg reduced hsCRP by approximately 38% from baseline at 20 weeks, an effect that persisted throughout the study. This reduction is comparable in magnitude to what was achieved with canakinumab (an anti-IL-1β monoclonal antibody) in the CANTOS trial, which demonstrated that targeting inflammation alone reduces cardiovascular events.
The CRP reduction with GLP-1 RAs is not simply a reflection of weight loss. While adipose tissue is a significant source of inflammatory mediators, analyses controlling for changes in body weight show that GLP-1 RAs still produce CRP reductions exceeding those predicted by weight loss alone. In a pooled analysis of SUSTAIN trials, semaglutide reduced CRP by 25-40% even after statistical adjustment for body weight change, suggesting direct anti-inflammatory pharmacological activity.
Interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and interleukin-1 beta (IL-1β) are key pro-inflammatory cytokines that drive atherosclerotic progression. GLP-1 RAs reduce circulating levels of all three. Liraglutide treatment in the LEADER trial was associated with a 15-20% reduction in IL-6 levels at 36 months. In vitro, liraglutide directly suppresses NF-κB activation in macrophages, the master transcriptional regulator of inflammatory cytokine production. This occurs through a cAMP-PKA-dependent mechanism that inhibits IκB kinase (IKK), preventing the nuclear translocation of NF-κB and the subsequent transcription of IL-6, TNF-α, and IL-1β.
Fibrinogen and plasminogen activator inhibitor-1 (PAI-1) are inflammatory and prothrombotic markers that are also reduced by GLP-1 RA therapy. PAI-1 is produced by adipose tissue, endothelial cells, and hepatocytes, and elevated levels promote a prothrombotic state by inhibiting fibrinolysis. Semaglutide reduces PAI-1 levels by approximately 20-30%, which may contribute to a reduced risk of thrombotic events including myocardial infarction and ischemic stroke.
Macrophage Modulation and Foam Cell Formation
Macrophages are the central cellular mediators of atherosclerosis. Circulating monocytes recruited to the arterial wall differentiate into macrophages that ingest oxidized LDL, becoming lipid-laden "foam cells" that form the core of atherosclerotic plaques. GLP-1 receptors are expressed on human monocytes and macrophages, providing a direct target for pharmacological modulation of these critical immune cells.
GLP-1 receptor activation shifts macrophage polarization from the pro-inflammatory M1 phenotype toward the anti-inflammatory M2 phenotype. M1 macrophages produce large quantities of TNF-α, IL-6, and reactive oxygen species, promoting tissue damage and plaque instability. M2 macrophages, by contrast, produce anti-inflammatory cytokines like IL-10 and TGF-β and promote tissue repair. In aortic plaques from ApoE-knockout mice treated with liraglutide, the M2/M1 macrophage ratio increased by approximately 2.5-fold compared to vehicle-treated controls.
Foam cell formation is directly inhibited by GLP-1R activation. Liraglutide and semaglutide reduce macrophage expression of scavenger receptors CD36 and LOX-1, which mediate the uptake of oxidized LDL. Simultaneously, GLP-1 RAs upregulate ABCA1 and ABCG1 transporters that promote cholesterol efflux from macrophages, effectively reversing the lipid accumulation that defines foam cell pathology. In one study using human monocyte-derived macrophages, exenatide reduced foam cell formation by 45% when cells were exposed to oxidized LDL for 24 hours.
The NLRP3 inflammasome, a multiprotein complex that activates IL-1β and IL-18, has emerged as a critical mediator of atherosclerotic inflammation. Cholesterol crystals deposited in plaques activate the NLRP3 inflammasome, triggering a self-amplifying inflammatory cascade. GLP-1 receptor agonists suppress NLRP3 inflammasome assembly in macrophages through a cAMP-dependent mechanism. This effect has been demonstrated in both murine peritoneal macrophages and human THP-1 cells, with liraglutide reducing NLRP3 protein expression by approximately 50% and caspase-1 activity by 40%.
T Cell and Adaptive Immune Modulation
While macrophages dominate the innate immune response in atherosclerosis, T cells of the adaptive immune system also play significant roles. Th1 cells and their signature cytokine interferon-gamma (IFN-γ) promote plaque inflammation and instability, while regulatory T cells (Tregs) suppress inflammation and stabilize plaques. GLP-1 receptors are expressed on T cells, and receptor activation appears to shift the Th1/Treg balance in favor of immune regulation.
In a study of patients with type 2 diabetes treated with liraglutide for 26 weeks, circulating Treg numbers increased by 18% while Th1 cells decreased by 12%, resulting in a significantly improved Th1/Treg ratio. This immunomodulatory effect was independent of changes in HbA1c or body weight and was not observed in patients treated with sulfonylureas as an active comparator. The mechanism involves cAMP-mediated enhancement of Foxp3 expression, the transcription factor that defines the Treg lineage.
Natural killer T (NKT) cells, which are enriched in atherosclerotic plaques and promote plaque vulnerability through production of IFN-γ and perforin, are also modulated by GLP-1R signaling. Exenatide treatment in ApoE-knockout mice reduced NKT cell infiltration into aortic plaques by approximately 35%, an effect associated with reduced plaque necrotic core size and increased fibrous cap thickness.
Plaque Stabilization and Regression
The most clinically relevant question is whether GLP-1 RAs can stabilize vulnerable plaques or promote plaque regression. Vulnerable plaques, characterized by large lipid-rich necrotic cores, thin fibrous caps, and heavy inflammatory cell infiltration, are responsible for the majority of acute coronary syndromes. Several lines of evidence suggest that GLP-1 receptor agonists favorably modify plaque composition.
In the ApoE-knockout mouse model of atherosclerosis, treatment with liraglutide for 12 weeks reduced aortic plaque area by 25-30% compared to vehicle. More significant than the reduction in plaque size was the change in plaque composition: liraglutide-treated mice showed a 40% increase in fibrous cap thickness, a 35% reduction in necrotic core area, and a 50% reduction in intraplaque hemorrhage. These changes collectively indicate a shift from vulnerable to stable plaque morphology.
Human imaging studies provide corroborating evidence. A small but well-designed study using carotid MRI in 35 patients with type 2 diabetes treated with liraglutide for 48 weeks showed a 12% reduction in carotid wall volume and a shift in plaque signal intensity consistent with reduced lipid content. A larger study using coronary CT angiography in 120 patients treated with semaglutide versus placebo for 12 months found that semaglutide reduced total coronary plaque volume by 8.2%, with a preferential reduction in non-calcified (lipid-rich) plaque. The shift from lipid-rich to calcified plaque is considered a marker of plaque stabilization.
Intraplaque angiogenesis, the formation of new blood vessels within the plaque, is a marker of plaque vulnerability and a source of intraplaque hemorrhage. GLP-1 RAs inhibit pathological angiogenesis through reduction of VEGF expression in plaque macrophages and through direct anti-angiogenic effects on endothelial cells. Semaglutide reduced VEGF-positive area within coronary plaques by 30% in a porcine model of accelerated atherosclerosis.
Oxidative Stress Reduction
Oxidative stress is both a cause and consequence of atherosclerosis. Reactive oxygen species (ROS) oxidize LDL particles, making them more atherogenic; activate NF-κB-dependent inflammatory pathways; impair endothelial NO bioavailability; and promote VSMC proliferation. GLP-1 receptor agonists reduce oxidative stress through several converging mechanisms.
NADPH oxidase (NOX), the primary enzymatic source of superoxide in the vasculature, is inhibited by GLP-1R signaling. In human aortic endothelial cells, liraglutide reduced NOX4 expression by 35% and NOX2 activity by 28%, with corresponding reductions in superoxide production and hydrogen peroxide levels. This effect was mediated through PKA-dependent inhibition of Rac1, a small GTPase required for NOX assembly.
Simultaneously, GLP-1 RAs enhance antioxidant defenses. Nuclear factor erythroid 2-related factor 2 (Nrf2), the master transcriptional regulator of antioxidant gene expression, is activated by GLP-1R signaling. Nrf2 target genes including heme oxygenase-1 (HO-1), superoxide dismutase (SOD), and glutathione peroxidase (GPx) are all upregulated in vascular tissues from GLP-1 RA-treated animals. In patients with type 2 diabetes, 12 weeks of exenatide treatment increased plasma SOD activity by 22% and reduced malondialdehyde (a lipid peroxidation marker) by 18%, indicating reduced systemic oxidative stress.
The combined effect of reduced ROS production and enhanced antioxidant capacity leads to improved NO bioavailability, better endothelial function, reduced LDL oxidation, and suppressed inflammatory signaling. These anti-oxidative effects work complementaryally with the direct anti-inflammatory and anti-atherosclerotic mechanisms to provide comprehensive vascular protection. For more information about the complete pharmacological profile, see our semaglutide complete guide.
Endothelial Glycocalyx Protection
The endothelial glycocalyx is a gel-like layer of proteoglycans and glycosaminoglycans that lines the luminal surface of blood vessels. This structure acts as a mechanosensor for shear stress, a barrier to plasma protein and inflammatory cell infiltration, and a reservoir for protective enzymes including superoxide dismutase. Glycocalyx degradation is an early event in atherosclerosis and is accelerated by hyperglycemia, inflammation, and oxidative stress.
Emerging evidence suggests that GLP-1 RAs protect the endothelial glycocalyx. In a study using sublingual darkfield microscopy, 12 weeks of liraglutide treatment improved the perfused boundary region (a measure of glycocalyx thickness) by 15% in patients with type 2 diabetes. In vitro, semaglutide attenuated glycocalyx shedding induced by TNF-α in human coronary artery endothelial cells, an effect mediated through inhibition of heparanase, the enzyme primarily responsible for glycocalyx degradation. Protection of the glycocalyx may represent yet another mechanism through which GLP-1 RAs maintain vascular health and resist the initiation of atherosclerotic lesions.
Clinical Pearl
The anti-inflammatory effects of GLP-1 RAs operate at multiple levels: systemic (CRP, IL-6, TNF-α reduction), cellular (macrophage polarization, foam cell inhibition, T cell modulation), and vascular (endothelial protection, plaque stabilization, antioxidant enhancement). This multi-layered anti-inflammatory action distinguishes GLP-1 RAs from single-target anti-inflammatory therapies and may explain the consistency and magnitude of cardiovascular benefit observed across clinical trials. The roughly 40% reduction in CRP achieved with semaglutide approaches the effect size seen with dedicated anti-inflammatory agents like canakinumab.
CVOT Results Across the GLP-1 Class
Six major cardiovascular outcomes trials have evaluated GLP-1 receptor agonists in patients at elevated cardiovascular risk. Four of these trials demonstrated statistically significant reductions in the primary composite endpoint of three-point MACE (cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke), while the remaining two showed numerical trends toward benefit. Together, these trials represent one of the most compelling bodies of evidence for any cardiovascular risk reduction strategy developed in the past decade.
The FDA CVOT Mandate
The story begins in 2008, when the FDA issued guidance requiring all new antidiabetic drugs to demonstrate cardiovascular safety through dedicated outcomes trials. This mandate followed the controversy surrounding rosiglitazone, a thiazolidinedione linked to increased myocardial infarction risk. The requirement was initially viewed as a regulatory burden, a high bar that would slow drug approval without yielding useful therapeutic insights. That assumption proved spectacularly wrong for the GLP-1 class.
Each GLP-1 receptor agonist was required to undergo a large, randomized, placebo-controlled trial with adjudicated cardiovascular events as the primary endpoint. The trials were designed to rule out excess cardiovascular risk (non-inferiority), but several went on to demonstrate superiority. This transformation from safety trials to efficacy trials fundamentally changed how GLP-1 receptor agonists are prescribed and positioned in treatment algorithms.
LEADER: Liraglutide (2016)
The Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial was the first GLP-1 RA CVOT to demonstrate cardiovascular superiority. Published in the New England Journal of Medicine in 2016, LEADER randomized 9,340 patients with type 2 diabetes and high cardiovascular risk to liraglutide 1.8 mg daily or placebo, on top of standard care. The median follow-up was 3.8 years.
The primary endpoint of three-point MACE occurred in 13.0% of the liraglutide group versus 14.9% of the placebo group, yielding a hazard ratio of 0.87 (95% CI: 0.78-0.97, P=0.01 for superiority). This 13% relative risk reduction was driven primarily by a significant reduction in cardiovascular death (HR 0.78, 95% CI: 0.66-0.93). Non-fatal MI showed a non-significant trend toward benefit (HR 0.88), and non-fatal stroke was neutral (HR 0.89).
All-cause mortality was also significantly reduced (HR 0.85, 95% CI: 0.74-0.97), making LEADER one of the few diabetes trials to demonstrate a mortality benefit. The number needed to treat (NNT) to prevent one MACE event over 3.8 years was 53, and the NNT to prevent one cardiovascular death was 71. Subgroup analyses showed consistent benefit across age, sex, baseline HbA1c, duration of diabetes, and presence of established cardiovascular disease versus risk factors only.
SUSTAIN-6: Subcutaneous Semaglutide (2016)
SUSTAIN-6 was a pre-approval CVOT for subcutaneous semaglutide that enrolled 3,297 patients with type 2 diabetes and established cardiovascular disease or cardiovascular risk factors. Unlike LEADER, SUSTAIN-6 was designed primarily as a non-inferiority trial, and its relatively smaller sample size reflected this more limited objective. Despite this, the results exceeded expectations.
Three-point MACE occurred in 6.6% of the semaglutide group versus 8.9% of the placebo group over a median follow-up of 2.1 years (HR 0.74, 95% CI: 0.58-0.95, P=0.02 for superiority). The 26% relative risk reduction was the largest observed in any GLP-1 RA CVOT at that time. The benefit was driven by a striking 39% reduction in non-fatal stroke (HR 0.61, 95% CI: 0.38-0.99) and a 26% reduction in non-fatal MI (HR 0.74, 95% CI: 0.51-1.08, not statistically significant). Cardiovascular death was numerically lower but not statistically significant (HR 0.98).
The stroke reduction in SUSTAIN-6 was particularly notable and has been the subject of considerable discussion. Some researchers have suggested that GLP-1 RAs may have specific anti-atherosclerotic effects on carotid and cerebrovascular plaque, beyond their coronary benefits. The blood pressure reduction (4.5 mmHg systolic) and potential anti-inflammatory effects on cerebral vasculature may also contribute to stroke prevention.
REWIND: Dulaglutide (2019)
The Researching Cardiovascular Events with a Weekly Incretin in Diabetes (REWIND) trial differed from earlier CVOTs in its inclusion criteria. While LEADER and SUSTAIN-6 enrolled patients with established CVD or very high risk, REWIND included a broader population: 9,901 patients with type 2 diabetes, of whom only 31% had established cardiovascular disease. The remainder had cardiovascular risk factors only. This design allowed REWIND to assess GLP-1 RA efficacy in a primary prevention context.
Over a median follow-up of 5.4 years (the longest of any GLP-1 CVOT), dulaglutide 1.5 mg weekly reduced three-point MACE by 12% (HR 0.88, 95% CI: 0.79-0.99, P=0.026). The benefit was consistent between patients with and without established CVD, suggesting that GLP-1 RAs provide cardiovascular protection even in lower-risk populations. Non-fatal stroke was significantly reduced (HR 0.76, 95% CI: 0.61-0.95), consistent with the stroke signal seen in SUSTAIN-6. Cardiovascular death (HR 0.91) and non-fatal MI (HR 0.96) showed non-significant trends.
REWIND's importance lies in its demonstration that cardiovascular protection extends to primary prevention populations. The baseline HbA1c was 7.3% (lower than in LEADER or SUSTAIN-6), the baseline cardiovascular risk was more moderate, and the majority of patients did not have established atherosclerotic disease. Yet dulaglutide still delivered meaningful MACE reduction. This broadened the evidence base and supported wider guideline recommendations.
EXSCEL: Extended-Release Exenatide (2017)
The Exenatide Study of Cardiovascular Event Lowering (EXSCEL) evaluated extended-release exenatide 2 mg weekly in 14,752 patients with type 2 diabetes. This was the largest GLP-1 RA CVOT by enrollment. Over a median follow-up of 3.2 years, the primary MACE endpoint showed a non-significant 9% reduction (HR 0.91, 95% CI: 0.83-1.00, P=0.06). The result technically met the pre-specified non-inferiority criterion but missed superiority.
Several factors may explain EXSCEL's neutral result. The trial had a high discontinuation rate (43% in the exenatide group stopped study drug), which diluted the treatment effect in the intention-to-treat analysis. In a modified analysis excluding patients who discontinued early, the MACE reduction was more pronounced. The drug's relatively shorter half-life and lower GLP-1R occupancy compared to liraglutide and semaglutide may also have contributed to a smaller effect size. All-cause mortality was significantly lower with exenatide (HR 0.86, P=0.016), driven by a reduction in non-cardiovascular deaths.
PIONEER 6: Oral Semaglutide (2019)
PIONEER 6 tested oral semaglutide 14 mg daily in 3,183 patients with type 2 diabetes and high cardiovascular risk. As a pre-approval safety trial, it was not powered to detect superiority for MACE. The primary endpoint showed a non-significant 21% reduction (HR 0.79, 95% CI: 0.57-1.11, P=0.17 for superiority). Cardiovascular death was significantly lower (HR 0.49, 95% CI: 0.27-0.92), an unexpected finding in a trial of this size.
The large cardiovascular death reduction in PIONEER 6 has been interpreted cautiously given the small absolute number of events and wide confidence interval. The SOUL trial (Semaglutide Oral Cardiovascular Outcomes in Patients with Type 2 Diabetes), specifically designed and powered to assess cardiovascular efficacy of oral semaglutide, completed enrollment and reported results in late 2024, confirming significant MACE reduction with oral semaglutide 14 mg.
SELECT: Semaglutide for Cardiovascular Risk (2023)
The Semaglutide Effects on Cardiovascular Outcomes in People with Overweight or Obesity (SELECT) trial represents a paradigm in GLP-1 RA cardiovascular research. Enrolling 17,604 non-diabetic adults aged 45+ with BMI ≥27 and established atherosclerotic CVD, SELECT was the first CVOT to test a GLP-1 RA specifically for cardiovascular risk reduction in a non-diabetic population. Semaglutide 2.4 mg weekly reduced three-point MACE by 20% (HR 0.80, 95% CI: 0.72-0.90, P<0.001). The SELECT trial is covered in detail in the next section.
MACE Hazard Ratios Across GLP-1 CVOTs (vs Placebo)
Cross-Trial Comparison and Meta-Analyses
| Trial | Drug | N | Population | Median F/U | MACE HR (95% CI) | CV Death HR |
|---|---|---|---|---|---|---|
| LEADER | Liraglutide 1.8mg QD | 9,340 | T2D + high CV risk | 3.8 yr | 0.87 (0.78-0.97) | 0.78 (0.66-0.93) |
| SUSTAIN-6 | Semaglutide 0.5/1.0mg QW | 3,297 | T2D + CVD/risk | 2.1 yr | 0.74 (0.58-0.95) | 0.98 (0.65-1.48) |
| REWIND | Dulaglutide 1.5mg QW | 9,901 | T2D + CVD/risk (31% CVD) | 5.4 yr | 0.88 (0.79-0.99) | 0.91 (0.78-1.06) |
| EXSCEL | Exenatide ER 2mg QW | 14,752 | T2D (73% CVD) | 3.2 yr | 0.91 (0.83-1.00) | 0.88 (0.76-1.02) |
| PIONEER 6 | Oral semaglutide 14mg QD | 3,183 | T2D + high CV risk | 1.3 yr | 0.79 (0.57-1.11) | 0.49 (0.27-0.92) |
| SELECT | Semaglutide 2.4mg QW | 17,604 | Obese + ASCVD (no DM) | 3.3 yr | 0.80 (0.72-0.90) | 0.85 (0.71-1.01) |
A meta-analysis published in The Lancet Diabetes & Endocrinology pooling data from all six GLP-1 RA CVOTs found a combined MACE hazard ratio of 0.86 (95% CI: 0.80-0.93), with no significant heterogeneity across trials (I² = 28%). This corresponds to a 14% reduction in MACE. Individual MACE components showed varying degrees of reduction: non-fatal stroke was reduced by 17% (HR 0.83), non-fatal MI by 9% (HR 0.91), and cardiovascular death by 12% (HR 0.88). All-cause mortality was reduced by 12% (HR 0.88, 95% CI: 0.82-0.94).
Subgroup analyses from the meta-analysis revealed several important patterns. First, the cardiovascular benefit was consistent regardless of baseline HbA1c, suggesting that glycemic control is not the primary mediator of cardioprotection. Second, patients with established CVD derived greater absolute benefit than those with risk factors only, though relative risk reductions were similar. Third, the magnitude of benefit was numerically larger with GLP-1 RAs that have a human GLP-1 backbone (liraglutide, semaglutide, dulaglutide) compared to exendin-4-based agents (exenatide), though this difference did not reach statistical significance.
The consistency of cardiovascular benefit across different molecules, populations, and trial designs is perhaps the strongest argument that GLP-1 receptor agonism itself confers cardiovascular protection. This isn't a drug-specific effect or a statistical anomaly in a single trial. It's a class effect supported by over 60,000 patient-years of randomized, placebo-controlled evidence. For a broader comparison of different GLP-1 agents, see our GLP-1 class overview.
Key Finding
Across all six CVOTs, the pooled MACE reduction of 14% translates to approximately 14 fewer cardiovascular events per 1,000 patient-years of treatment. The consistency across trials (I² = 28%) strongly supports a true class effect rather than a drug-specific or chance finding. The benefit extends from high-risk secondary prevention populations (LEADER, SELECT) to lower-risk primary prevention populations (REWIND), and from diabetic to non-diabetic patients.
SELECT Trial Detailed look
The SELECT trial fundamentally changed how we think about GLP-1 receptor agonists and cardiovascular disease. By demonstrating that semaglutide 2.4 mg reduces MACE by 20% in non-diabetic patients with obesity and established cardiovascular disease, SELECT decoupled the cardiovascular benefits of GLP-1 RAs from diabetes management and established them as standalone cardiovascular risk reduction agents.
Trial Design and Rationale
SELECT was a randomized, double-blind, placebo-controlled, event-driven superiority trial conducted at 804 sites across 41 countries. The trial was sponsored by Novo Nordisk and registered as NCT03574597. Enrollment began in October 2018 and the primary results were presented at the American Heart Association Scientific Sessions in November 2023, with simultaneous publication in the New England Journal of Medicine.
The rationale for SELECT was straightforward: previous CVOTs had shown GLP-1 RA cardiovascular benefit in diabetic populations, and mediation analyses suggested that only a fraction of this benefit was explained by glycemic improvement. If GLP-1 RAs protect the heart through weight loss, anti-inflammatory effects, and direct vascular actions, then non-diabetic patients with obesity and cardiovascular disease should also benefit. SELECT was designed to test this hypothesis directly.
The study enrolled adults aged 45 years or older with a BMI of 27 kg/m² or greater and established atherosclerotic cardiovascular disease (prior myocardial infarction, prior stroke, or symptomatic peripheral arterial disease). Patients with diabetes (type 1 or type 2) or HbA1c ≥6.5% were excluded. Other exclusion criteria included planned coronary or peripheral revascularization, NYHA class IV heart failure, and end-stage renal disease.
Participants were randomized 1:1 to subcutaneous semaglutide 2.4 mg weekly (following a standard dose-escalation protocol starting at 0.24 mg weekly) or matching placebo. Background cardiovascular medications including statins, antihypertensives, and antiplatelets were continued per standard of care. The dose-escalation schedule reached the target dose of 2.4 mg at week 16, the same schedule used in the STEP weight management trials.
Baseline Characteristics
The 17,604 randomized participants had a mean age of 61.6 years, 72% were male, and the mean BMI was 33.3 kg/m². The qualifying cardiovascular event was prior MI in 70%, prior stroke in 18%, and symptomatic PAD in 18% (some had more than one qualifying condition). The mean HbA1c was 5.8%, confirming the non-diabetic status. Background therapy was strong: 90% were on statins, 86% on antiplatelets, 82% on antihypertensives, and 32% on beta-blockers.
This was a well-treated population already receiving guideline-directed medical therapy. Any cardiovascular benefit from semaglutide would be incremental, on top of statins, aspirin, ACE inhibitors, and other proven therapies. This makes the 20% MACE reduction even more impressive - it was achieved in a context where the residual cardiovascular risk was already being aggressively managed.
Primary Endpoint Results
The primary endpoint of three-point MACE occurred in 569 of 8,803 patients (6.5%) in the semaglutide group versus 701 of 8,801 patients (8.0%) in the placebo group, yielding a hazard ratio of 0.80 (95% CI: 0.72-0.90, P<0.001). The Kaplan-Meier curves separated early, with visible divergence apparent by 6 months and continuing to widen throughout the follow-up period. The median follow-up was 39.8 months (interquartile range 30.2-49.7).
Breaking down the individual MACE components:
- Cardiovascular death: HR 0.85 (95% CI: 0.71-1.01, P=0.07) - numerically favored but did not reach statistical significance
- Non-fatal myocardial infarction: HR 0.72 (95% CI: 0.61-0.85, P<0.001) - 28% reduction, statistically significant
- Non-fatal stroke: HR 0.93 (95% CI: 0.74-1.15, P=0.49) - non-significant
The MACE benefit in SELECT was driven predominantly by the reduction in non-fatal MI, which contrasts with SUSTAIN-6 where the benefit was stroke-driven. This difference may reflect the different patient populations (established CVD versus mixed CVD/risk factors) or could be a chance variation given that individual MACE components have wider confidence intervals. The important point is that the composite MACE endpoint was clearly and strongly reduced.
Secondary and Exploratory Endpoints
Several secondary endpoints provided additional support for the cardiovascular benefit of semaglutide in SELECT:
- All-cause death: HR 0.81 (95% CI: 0.71-0.93) - 19% reduction
- Coronary revascularization: HR 0.79 (95% CI: 0.70-0.89)
- Composite of cardiovascular death, non-fatal MI, non-fatal stroke, or coronary revascularization (4-point MACE): HR 0.78 (95% CI: 0.71-0.85)
- Heart failure composite (CV death or hospitalization/urgent visit for HF): HR 0.82 (95% CI: 0.71-0.96)
The 19% reduction in all-cause mortality is particularly striking and, if confirmed in additional analyses and trials, would make semaglutide one of the few pharmacological interventions shown to reduce mortality in this population beyond what's achieved with standard care. The coronary revascularization reduction suggests that semaglutide may slow the progression of coronary atherosclerosis, reducing the need for bypass surgery and percutaneous coronary intervention.
Weight Loss and Metabolic Effects
At 104 weeks, participants in the semaglutide group lost a mean of 9.4% of their body weight compared to 0.9% in the placebo group, a between-group difference of 8.5 percentage points. This is consistent with the weight loss magnitude observed in the STEP program. Waist circumference decreased by 7.7 cm with semaglutide versus 1.3 cm with placebo.
Systolic blood pressure decreased by 3.8 mmHg more with semaglutide than placebo. HsCRP decreased by 37.8% with semaglutide versus a slight increase with placebo. Triglycerides improved by 16% more with semaglutide. LDL cholesterol showed minimal change, which is not surprising given that 90% of patients were already on statins.
Mediation Analyses
A pre-specified mediation analysis examined what proportion of the MACE reduction could be attributed to changes in body weight versus other factors. This analysis estimated that approximately 40% of the treatment effect on MACE was mediated through body weight reduction. The remaining 60% was attributed to weight-independent mechanisms, including direct anti-inflammatory effects (CRP mediated approximately 22% of the benefit), improvements in blood pressure, changes in waist circumference beyond what weight loss alone would predict, and presumed direct vascular effects not captured by measured biomarkers.
This mediation analysis has significant clinical implications. It means that even if a patient on semaglutide achieves modest weight loss, they may still derive substantial cardiovascular benefit from the drug's non-weight-mediated mechanisms. It also suggests that the cardiovascular benefit of GLP-1 RAs is mechanistically distinct from, and potentially additive to, the cardiovascular benefit of lifestyle-based weight management. For more on the weight loss aspects of GLP-1 therapy, see our weight loss mechanisms guide.
Subgroup Analyses
SELECT's subgroup analyses demonstrated remarkably consistent benefit across pre-specified subgroups. The 20% MACE reduction was maintained regardless of:
- Age (45-54 vs 55-64 vs ≥65 years)
- Sex (men vs women, though the trial was 72% male)
- Race (White, Black, Asian, other)
- Baseline BMI (27-30 vs 30-35 vs ≥35 kg/m²)
- Baseline HbA1c (above or below median of 5.8%)
- Type of qualifying CVD event (MI, stroke, PAD)
- Statin use at baseline
- Baseline eGFR
One subgroup finding of particular interest: patients with a baseline HbA1c of 5.7-6.4% (prediabetes range) showed a similar MACE benefit to those with HbA1c below 5.7%. And among patients who developed new-onset diabetes during the trial (fewer in the semaglutide group), the MACE benefit was consistent. These findings reinforce the conclusion that glycemic status is not a meaningful modifier of GLP-1 RA cardiovascular benefit.
Safety Profile in SELECT
The safety profile of semaglutide 2.4 mg in SELECT was consistent with what's been observed in previous trials. Gastrointestinal adverse events were the most common treatment-related complaints: nausea (44% vs 26%), diarrhea (30% vs 17%), vomiting (24% vs 8%), and constipation (22% vs 12%). These events were generally mild to moderate, occurred primarily during the dose-escalation phase, and led to permanent drug discontinuation in 16.6% of the semaglutide group versus 8.2% of the placebo group.
Gallbladder-related events occurred in 2.8% of semaglutide patients versus 2.3% of placebo patients. Pancreatitis was reported in 0.2% versus 0.1%, a small absolute difference. There was no signal for thyroid cancer, pancreatic cancer, or other malignancies. Heart rate increased by a mean of 3.0 bpm with semaglutide compared to 0.2 bpm with placebo, consistent with the class effect.
Serious adverse events were balanced between groups (33.4% semaglutide vs 36.4% placebo), and the lower rate in the semaglutide group likely reflects the cardiovascular protection. The overall benefit-risk profile strongly favored semaglutide, with the 20% MACE reduction far outweighing the gastrointestinal side effect burden.
SELECT in Context
SELECT is one of the largest and most impactful cardiovascular outcomes trials ever conducted. The 20% MACE reduction in non-diabetic obese patients with established ASCVD has three major implications: (1) GLP-1 RA cardiovascular benefit is not limited to diabetes; (2) the benefit is partly independent of weight loss and glycemic control; (3) semaglutide 2.4 mg should be considered a cardiovascular risk reduction agent in its own right, alongside statins, antihypertensives, and antiplatelets. The trial has prompted FDA and EMA label expansions and is reshaping guideline recommendations.
Heart Failure Outcomes
Heart failure with preserved ejection fraction (HFpEF) has long been called the "unmet need" of cardiovascular medicine. Unlike heart failure with reduced ejection fraction (HFrEF), which has multiple evidence-based pharmacological therapies, HFpEF lacked effective drug treatments for decades. Obesity and metabolic dysfunction are major drivers of HFpEF, making GLP-1 receptor agonists a logical therapeutic target. Recent trial data have validated this hypothesis with striking results.
The Obesity-HFpEF Connection
More than 80% of patients with HFpEF are overweight or obese. Excess adiposity contributes to HFpEF through multiple mechanisms: increased blood volume and cardiac preload, systemic inflammation (particularly from epicardial and pericardial fat), insulin resistance causing impaired myocardial energetics, and direct lipotoxic effects on cardiomyocytes. Epicardial adipose tissue, which directly surrounds the heart and shares its blood supply, produces inflammatory cytokines including IL-6, TNF-α, and adipokines that promote myocardial fibrosis, diastolic dysfunction, and impaired relaxation.
Patients with obesity-related HFpEF represent a distinct phenotype characterized by greater symptom burden, worse exercise capacity, higher filling pressures, and a hemodynamic profile dominated by plasma volume expansion. These patients typically have elevated levels of natriuretic peptides (though sometimes "relatively" low given their degree of congestion, due to the natriuretic peptide-lowering effect of obesity), higher CRP, and more pronounced diastolic dysfunction.
Weight loss through any means improves HFpEF symptoms and hemodynamics. Bariatric surgery studies have demonstrated dramatic improvements in filling pressures, exercise capacity, and quality of life. But bariatric surgery carries procedural risk and is not feasible for most HFpEF patients, particularly the elderly. Pharmacological weight loss with GLP-1 RAs offers a more accessible approach, with the added advantage of direct anti-inflammatory and cardioprotective effects beyond weight reduction alone.
STEP-HFpEF: Semaglutide in Obesity-Related HFpEF
The STEP-HFpEF trial (Semaglutide Treatment Effect in People with obesity and HFpEF) was a randomized, double-blind, placebo-controlled trial that enrolled 529 patients with HFpEF, a left ventricular ejection fraction of ≥45%, and a BMI of ≥30 kg/m². Participants were randomized to semaglutide 2.4 mg weekly or placebo for 52 weeks. Patients with diabetes were excluded (a companion trial, STEP-HFpEF DM, enrolled diabetic patients).
The trial had two primary endpoints: the change in the Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS, a validated measure of heart failure symptoms and physical limitations) and the change in body weight. Semaglutide improved KCCQ-CSS by 7.8 points more than placebo (16.6 vs 8.7 points; P<0.001). To put this in perspective, a 5-point change in KCCQ-CSS is considered clinically meaningful. The 7.8-point between-group difference is large by heart failure trial standards and was perceived by patients as a substantial improvement in daily functioning.
Body weight decreased by 13.3% with semaglutide versus 2.6% with placebo (between-group difference: -10.7 percentage points). The 6-minute walk distance improved by 21.5 meters more with semaglutide, a meaningful functional improvement. CRP decreased by 43.5% from baseline with semaglutide versus an 8% reduction with placebo, confirming the anti-inflammatory effect in this population.
In a hierarchical composite endpoint analysis (death, heart failure events, KCCQ-CSS change, and 6-minute walk distance), semaglutide was superior to placebo (win ratio 1.72, P<0.001). Heart failure events (hospitalizations or urgent visits) occurred in 4 patients (1.5%) in the semaglutide group versus 10 patients (3.8%) in the placebo group. While these numbers are small and the trial was not powered for hard endpoints, the direction is consistent with a clinically meaningful reduction in HF morbidity.
STEP-HFpEF DM
The companion STEP-HFpEF DM trial enrolled 616 patients with HFpEF, obesity, and type 2 diabetes. Results were similar: semaglutide improved KCCQ-CSS by 7.3 points more than placebo and reduced body weight by 6.4% more than placebo. The smaller weight loss difference in the diabetic cohort (6.4% vs 10.7% in non-diabetic STEP-HFpEF) is consistent with the observation that patients with diabetes tend to lose less weight on GLP-1 RAs, possibly due to insulin resistance-related metabolic differences.
the KCCQ improvement was nearly identical between the diabetic and non-diabetic trials (7.3 vs 7.8 points), despite the smaller weight differential. This observation suggests that a substantial portion of the heart failure symptom benefit is independent of weight loss magnitude and may be driven by anti-inflammatory effects, reduced epicardial fat, improved diastolic function, and other direct mechanisms.
SUMMIT: Tirzepatide in HFpEF
The SUMMIT trial evaluated tirzepatide, a dual GIP/GLP-1 receptor agonist, in patients with HFpEF and obesity. This trial enrolled 731 patients and followed them for up to 104 weeks, making it the longest and most strongly powered HFpEF trial in this space. Unlike STEP-HFpEF, SUMMIT included a pre-specified composite primary endpoint of cardiovascular death or a worsening heart failure event (hospitalization or urgent visit).
Tirzepatide reduced the composite primary endpoint by 38% (HR 0.62, 95% CI: 0.41-0.95, P=0.026). This was driven by a 56% reduction in worsening heart failure events (HR 0.44, 95% CI: 0.26-0.75). Cardiovascular death was numerically lower with tirzepatide but not individually significant given the small number of events. KCCQ-CSS improved by 6.9 points more with tirzepatide, and body weight decreased by 11.6% more than placebo.
SUMMIT's demonstration of a reduction in hard cardiovascular endpoints (not just symptoms) is a major advance for the field. It suggests that GLP-1-based therapies don't simply make HFpEF patients feel better. They actually reduce the risk of clinical deterioration and hospitalization. The 38% reduction in the composite endpoint is one of the largest treatment effects seen in any HFpEF trial and positions tirzepatide as a potential breakthrough therapy for this condition. For detailed information about tirzepatide, see our tirzepatide guide.
Mechanisms of Heart Failure Benefit
Several mechanisms contribute to the heart failure benefits observed with GLP-1 RAs and dual agonists:
Epicardial fat reduction. Cardiac MRI substudies from STEP-HFpEF show that semaglutide reduces epicardial adipose tissue volume by approximately 20% at 52 weeks. This reduction in pericardial fat directly decreases the local inflammatory burden on the myocardium, reduces mechanical compression of the heart, and improves diastolic compliance. The correlation between epicardial fat reduction and KCCQ improvement supports a causal relationship.
Plasma volume contraction. GLP-1 RAs promote natriuresis through direct effects on renal proximal tubular sodium reabsorption. This leads to a modest reduction in plasma volume that decreases cardiac preload and filling pressures. In hemodynamic studies, liraglutide reduced pulmonary capillary wedge pressure (PCWP) by 3-4 mmHg, an effect that directly alleviates pulmonary congestion and dyspnea.
Improved myocardial energetics. The failing heart is an "energy-starved" organ with impaired mitochondrial function and reduced ATP production. GLP-1 receptor activation improves myocardial glucose uptake and shifts substrate utilization toward more oxygen-efficient pathways. In PET studies, liraglutide increased myocardial glucose uptake by approximately 25% in patients with ischemic heart failure.
Reduced myocardial fibrosis. As discussed in the receptor biology section, GLP-1 RAs reduce cardiac fibrosis through suppression of TGF-β signaling. Cardiac MRI T1 mapping from STEP-HFpEF substudies shows reduced extracellular volume fraction (a marker of diffuse fibrosis) with semaglutide treatment, though these data are still preliminary.
Anti-inflammatory effects. The 40-45% reduction in CRP with semaglutide directly addresses the inflammatory pathophysiology of obesity-related HFpEF. Reduced systemic and cardiac inflammation improves endothelial function, reduces coronary microvascular dysfunction, and attenuates the pro-fibrotic signaling that drives diastolic impairment.
Heart Failure with Reduced Ejection Fraction (HFrEF)
The evidence for GLP-1 RAs in HFrEF is less developed. Earlier small trials of liraglutide in HFrEF (the FIGHT trial, N=300) showed no improvement in a combined clinical endpoint, though the trial was underpowered and used a lower dose. Post-hoc analyses from CVOTs suggest that the MACE reduction with GLP-1 RAs is preserved in patients with a history of heart failure, and heart failure hospitalization rates are generally lower in GLP-1 RA-treated groups.
The mechanism of benefit may differ between HFpEF and HFrEF. In HFpEF, the predominant pathophysiology is diastolic dysfunction driven by obesity, inflammation, and fibrosis, all directly targeted by GLP-1 RAs. In HFrEF, the pathophysiology centers on systolic dysfunction from myocardial injury, neurohormonal activation, and adverse remodeling. While GLP-1 RAs have theoretical benefits in HFrEF (improved energetics, reduced fibrosis, anti-apoptotic effects), the clinical evidence has not yet demonstrated meaningful benefit. Ongoing studies are exploring whether higher doses of semaglutide or tirzepatide might show efficacy in HFrEF, particularly in the obese HFrEF phenotype.
Clinical Pearl
STEP-HFpEF and SUMMIT have established GLP-1-based therapies as the first pharmacological treatments with strong evidence for improving outcomes in obesity-related HFpEF. The SUMMIT trial's 38% reduction in the composite of CV death and worsening HF events is particularly compelling because it demonstrates benefit on hard clinical endpoints, not just symptoms. For patients with HFpEF and a BMI ≥30, initiating a GLP-1 RA or dual agonist should now be considered part of standard care, alongside diuretics, SGLT2 inhibitors, and lifestyle modification.
Blood Pressure & Lipid Effects

Beyond the direct anti-atherosclerotic and anti-inflammatory mechanisms, GLP-1 receptor agonists improve several traditional cardiovascular risk factors. Blood pressure reductions, lipid profile changes, and improvements in metabolic syndrome components all contribute to the overall cardiovascular risk reduction. While none of these individual effects is dramatic, their cumulative impact is clinically meaningful.
Blood Pressure Reduction
Systolic blood pressure (SBP) consistently decreases by 3-6 mmHg with GLP-1 receptor agonist therapy, an effect observed across all major trials regardless of the specific agent used. In SELECT, semaglutide 2.4 mg reduced SBP by 3.8 mmHg more than placebo. In LEADER, liraglutide reduced SBP by 1.2 mmHg more than placebo (a smaller difference, partly because the control group also received antihypertensive therapy adjustments). In the STEP program (weight management trials), semaglutide 2.4 mg reduced SBP by 6-7 mmHg from baseline.
To put these numbers in context, a 5 mmHg sustained reduction in SBP is associated with approximately a 10% reduction in major cardiovascular events based on blood pressure meta-regression data. The blood pressure contribution to cardiovascular risk reduction with GLP-1 RAs is therefore modest but not negligible, accounting for an estimated 10-15% of the total MACE reduction observed in CVOTs.
The blood pressure lowering effect of GLP-1 RAs occurs through several converging mechanisms:
Natriuresis and volume reduction. GLP-1 receptor activation directly inhibits sodium-hydrogen exchanger 3 (NHE3) in the renal proximal tubule, reducing sodium reabsorption and promoting urinary sodium excretion. This natriuretic effect begins within hours of GLP-1 RA administration and leads to modest plasma volume contraction. In a study of healthy volunteers, a single dose of liraglutide increased 24-hour urinary sodium excretion by approximately 15%.
Vascular relaxation. As discussed earlier, GLP-1 receptor activation on endothelial cells stimulates NO production, and activation on vascular smooth muscle cells directly promotes relaxation through cAMP-mediated pathways. Flow-mediated dilation improves with GLP-1 RA therapy, reflecting enhanced endothelial vasodilatory capacity. These direct vascular effects contribute to reduced peripheral resistance and lower blood pressure.
Reduced sympathetic outflow. While central GLP-1 receptor activation modestly increases cardiac sympathetic tone (explaining the heart rate increase), peripheral sympathetic nerve activity to the vasculature appears to decrease with chronic GLP-1 RA treatment. Muscle sympathetic nerve activity (MSNA), measured by microneurography, decreased by 12% in a small study of liraglutide-treated hypertensive patients, contributing to reduced arterial tone.
Weight loss contribution. Weight loss itself reduces blood pressure through decreased blood volume, reduced sympathetic activation, and improved endothelial function. Approximately 50-60% of the blood pressure reduction with GLP-1 RAs is estimated to be weight-mediated, with the remainder attributable to the direct renal and vascular mechanisms described above. The rapid onset of blood pressure reduction (within 2-4 weeks) before significant weight loss has occurred supports the existence of weight-independent mechanisms.
RAAS modulation. GLP-1 RAs reduce circulating levels of angiotensin II and aldosterone, key hormones in the renin-angiotensin-aldosterone system that drive vasoconstriction, sodium retention, and cardiac remodeling. In patients with type 2 diabetes, 26 weeks of liraglutide treatment reduced plasma aldosterone by 18%, an effect that was independent of changes in serum potassium or renal function.
Diastolic blood pressure (DBP) also decreases with GLP-1 RA therapy, typically by 1-3 mmHg. While smaller than the systolic effect, the DBP reduction contributes to improved mean arterial pressure and reduced cardiac afterload. Pulse pressure (the difference between SBP and DBP) tends to narrow with treatment, suggesting improvement in arterial compliance and reduced arterial stiffness.
Lipid Profile Changes
GLP-1 receptor agonists produce modest but favorable changes in lipid profiles. The effects vary by lipid fraction:
Triglycerides. The most consistent lipid effect is a reduction in fasting triglycerides, typically in the range of 10-25% from baseline. In SELECT, semaglutide reduced triglycerides by 16% more than placebo. In SUSTAIN trials, semaglutide 1.0 mg reduced triglycerides by 12-22%. This triglyceride-lowering effect is partly mediated by weight loss (adipose tissue lipolysis decreases with reduced fat mass) and partly by direct hepatic effects. GLP-1 RAs reduce hepatic VLDL production by inhibiting de novo lipogenesis and stimulating fatty acid beta-oxidation in the liver. Reduced postprandial triglyceride excursions are also observed, reflecting delayed gastric emptying and improved chylomicron metabolism.
LDL cholesterol. Changes in LDL cholesterol with GLP-1 RAs are generally small (0-5% reduction). In many trials, LDL shows no significant change or a modest decrease. This minimal effect is expected, given that GLP-1 RAs don't directly target LDL receptor expression or cholesterol synthesis. In populations where 85-90% of patients are already on statins (as in SELECT), there is limited room for further LDL reduction. However, small dense LDL particles (a more atherogenic subfraction) may decrease disproportionately, contributing to cardiovascular benefit beyond what total LDL changes would predict.
HDL cholesterol. HDL cholesterol increases modestly by 1-5% with GLP-1 RA therapy. This effect is largely mediated by weight loss and improved insulin sensitivity. While the clinical significance of small HDL changes is debated, HDL functionality (cholesterol efflux capacity) may improve more than the quantitative HDL change suggests. A study using the cholesterol efflux assay showed that exenatide improved HDL efflux capacity by 8% in patients with type 2 diabetes, independent of changes in HDL-C concentration.
Free fatty acids and remnant lipoproteins. GLP-1 RAs reduce circulating free fatty acids (FFAs), which are toxic to cardiomyocytes in excess and promote insulin resistance. Remnant lipoproteins, triglyceride-rich particles that are strongly atherogenic, also decrease with GLP-1 RA therapy. These changes in atherogenic lipoproteins beyond LDL may contribute to cardiovascular risk reduction and help explain why MACE benefits exceed what LDL changes alone would predict.
Hepatic Fat and MASLD/MASH
GLP-1 RAs produce substantial reductions in hepatic fat content, measured by MRI-PDFF (proton density fat fraction). Semaglutide 2.4 mg reduces liver fat by 40-60% from baseline, with many patients achieving normalization of hepatic steatosis. This effect is highly relevant to cardiovascular risk because non-alcoholic fatty liver disease (now termed metabolic dysfunction-associated steatotic liver disease, or MASLD) is independently associated with accelerated atherosclerosis, coronary artery disease, and cardiovascular events.
The liver is the primary organ for lipoprotein metabolism, and hepatic steatosis promotes atherogenic dyslipidemia (high triglycerides, low HDL, increased small dense LDL). By reducing hepatic fat, GLP-1 RAs improve the metabolic milieu that drives dyslipidemia. Additionally, the fibrotic liver produces inflammatory mediators that contribute to systemic inflammation and endothelial dysfunction. Semaglutide's demonstrated ability to improve MASH (metabolic dysfunction-associated steatohepatitis) histology and reduce fibrosis staging, as shown in Phase 3 trials for the MASH indication, adds another dimension to its cardiovascular risk reduction profile.
Metabolic Syndrome Improvement
Metabolic syndrome, defined by the co-occurrence of abdominal obesity, hypertriglyceridemia, low HDL, hypertension, and hyperglycemia, affects approximately 35% of US adults and roughly doubles the risk of cardiovascular events. GLP-1 RAs address all five components of metabolic syndrome simultaneously:
| Metabolic Syndrome Component | Typical Effect with GLP-1 RA | Estimated Contribution to CV Risk Reduction |
|---|---|---|
| Waist circumference | ↓ 4-8 cm | Reduced visceral adiposity and inflammation |
| Triglycerides | ↓ 15-25% | Reduced atherogenic lipoprotein burden |
| HDL cholesterol | ↑ 1-5% | Improved reverse cholesterol transport |
| Blood pressure | ↓ 3-6 mmHg SBP | Reduced vascular strain and stroke risk |
| Fasting glucose | ↓ 5-15 mg/dL (non-diabetic) | Reduced glycemic toxicity to endothelium |
In SELECT, the proportion of patients meeting criteria for metabolic syndrome decreased from 78% at baseline to 56% at 104 weeks in the semaglutide group, compared to a decrease from 79% to 71% in the placebo group. This "metabolic syndrome resolution" effect means that semaglutide moved a substantial fraction of patients from a high-risk metabolic phenotype to a lower-risk one, with implications for long-term cardiovascular and diabetes risk.
Arterial Stiffness
Arterial stiffness, measured by pulse wave velocity (PWV) or augmentation index, is an independent predictor of cardiovascular events, particularly stroke and heart failure. Stiff arteries increase systolic pressure, increase cardiac afterload, and reduce coronary perfusion. GLP-1 RAs reduce arterial stiffness through their effects on endothelial function, vascular inflammation, and blood pressure. In a meta-analysis of 8 studies, GLP-1 RA therapy reduced carotid-femoral PWV by 0.6 m/s, a magnitude associated with a 10-15% reduction in cardiovascular event risk based on epidemiological data. This improvement in arterial compliance contributes to the blood pressure reduction and may independently reduce stroke and heart failure risk.
Integrated Risk Factor Management
No single risk factor change with GLP-1 RAs is large enough to explain the 12-26% MACE reduction observed in CVOTs. Rather, the cardiovascular benefit arises from the simultaneous, moderate improvement across multiple risk dimensions: blood pressure, triglycerides, inflammation (CRP), visceral fat, hepatic steatosis, arterial stiffness, and glucose metabolism. This "polypill-like" effect, combined with direct anti-atherosclerotic mechanisms, produces a cumulative cardiovascular benefit that exceeds the sum of individual risk factor changes.
Weight-Independent Cardioprotection
One of the most provocative findings from GLP-1 RA cardiovascular research is that the heart benefits substantially exceed what weight loss alone can explain. Multiple lines of evidence, from mediation analyses to time-course data to mechanistic studies, converge on the conclusion that GLP-1 receptor activation provides cardioprotection through pathways that operate independently of changes in body mass.
Mediation Analysis Evidence
Formal mediation analyses attempt to quantify how much of a treatment effect on an outcome (MACE) is "explained" by an intermediate variable (such as body weight change). In SELECT, a pre-specified mediation analysis estimated that changes in body weight mediated approximately 40% of the observed MACE reduction with semaglutide 2.4 mg. The remaining 60% was attributed to other, weight-independent mechanisms.
When additional mediators were included in the model, the picture became more nuanced. Changes in hsCRP mediated approximately 22% of the MACE benefit, changes in waist circumference (a proxy for visceral fat, which can change independently of total body weight) contributed approximately 12%, and changes in blood pressure accounted for roughly 8%. Even after accounting for all measured mediators, a substantial proportion of the MACE reduction (approximately 25-30%) remained unexplained, presumably reflecting direct vascular and cardiac effects that aren't captured by standard biomarkers.
Similar mediation analyses from LEADER estimated that only about 30% of the MACE benefit of liraglutide was mediated through HbA1c reduction, body weight, or their combination. In SUSTAIN-6, the 26% MACE reduction occurred despite relatively modest weight loss in the trial (4.3 kg difference), further supporting weight-independent mechanisms. And in REWIND, where the dulaglutide-placebo weight difference was only 1.5 kg, a 12% MACE reduction was still observed. If weight loss were the sole driver of cardiovascular benefit, the MACE reduction in REWIND should have been negligible given the minimal weight difference.
Time-Course Evidence
The timeline of cardiovascular benefit provides additional support for weight-independent mechanisms. In both LEADER and SELECT, Kaplan-Meier curves for MACE began to separate within the first 3-6 months of treatment. At 6 months in SELECT, semaglutide patients had lost approximately 6% of body weight, yet the event curves were already diverging. By contrast, the full magnitude of weight loss wasn't achieved until 60-68 weeks. If cardiovascular benefit were purely weight-mediated, we would expect a lag corresponding to the time required for substantial weight loss to accrue. The early separation of event curves suggests that mechanisms acting more rapidly than weight loss, such as anti-inflammatory effects and endothelial function improvement, are at play.
CRP reductions with semaglutide occur within the first 2-4 weeks of treatment, well before meaningful weight loss has occurred. In a pharmacokinetic/pharmacodynamic analysis from SUSTAIN-1, hsCRP decreased by 15% at week 4 when body weight had decreased by less than 1%. By week 12, CRP was reduced by approximately 30% while weight loss was still in the 3-4% range. This temporal dissociation between inflammatory marker improvement and weight loss supports the existence of a direct anti-inflammatory pharmacological effect.
Comparisons with Other Weight Loss Interventions
If GLP-1 RA cardiovascular benefits were solely weight-mediated, then other interventions producing equivalent weight loss should produce equivalent cardiovascular benefit. But this isn't consistently the case. Lifestyle interventions in the Look AHEAD trial (Action for Health in Diabetes) achieved a sustained weight loss difference of approximately 6% over 10 years in patients with type 2 diabetes and overweight/obesity. Despite this meaningful weight loss, Look AHEAD showed no significant reduction in cardiovascular events (HR 0.95 for the primary composite). Similarly, orlistat, a lipase inhibitor that produces modest weight loss (3-4% difference from placebo), has not demonstrated cardiovascular event reduction in any trial.
By contrast, semaglutide 2.4 mg in SELECT achieved a weight loss difference of 8.5% and a 20% MACE reduction. If we apply the weight-to-MACE mediation coefficient from SELECT (approximately 2.4% MACE reduction per 1% body weight lost), then the expected MACE reduction from 8.5% weight loss would be approximately 10%. The observed 20% reduction is roughly double the weight-predicted benefit, consistent with the mediation analysis estimate that 40% is weight-mediated.
Bariatric surgery studies provide another comparator. The Swedish Obese Subjects (SOS) study showed that bariatric surgery, which produces 15-25% sustained weight loss, reduces cardiovascular events by 30-40%. This is a larger effect than SELECT, but it's also achieved with much greater weight loss. The "cardiovascular benefit per unit weight loss" with semaglutide appears to exceed that achieved with surgical weight loss, again suggesting additive pharmacological mechanisms.
Direct Anti-Inflammatory Mechanisms
The strongest candidate for weight-independent cardioprotection is direct anti-inflammatory activity. As detailed in Section 3, GLP-1 RAs suppress NF-κB signaling, modulate macrophage polarization, inhibit the NLRP3 inflammasome, and reduce multiple circulating inflammatory biomarkers. These effects are mediated through GLP-1 receptors on immune cells and vascular tissue, not through changes in adipose mass.
The CANTOS trial (Canakinumab Anti-inflammatory Thrombosis Outcomes Study) demonstrated that targeting inflammation alone, with an anti-IL-1β monoclonal antibody, reduces MACE by 15% without any change in body weight, lipids, or blood pressure. This "proof of concept" for anti-inflammatory cardioprotection validates the biological plausibility that GLP-1 RAs' anti-inflammatory effects could independently reduce cardiovascular events. The magnitude of CRP reduction with semaglutide (approximately 38% in SELECT) is comparable to the CRP reduction achieved with canakinumab in CANTOS (approximately 30-40% depending on dose), providing a quantitative framework for estimating the anti-inflammatory contribution to MACE reduction.
Endothelial Function and Vascular Protection
Improved endothelial function is another weight-independent mechanism. While weight loss improves endothelial function through reduced inflammation and improved insulin sensitivity, GLP-1 RAs enhance endothelial NO bioavailability through direct receptor-mediated activation of eNOS. This effect has been demonstrated in normal-weight animals and in vitro systems where weight loss is not a factor, confirming a direct pharmacological mechanism.
In a crossover study of patients with type 2 diabetes, liraglutide improved flow-mediated dilation (FMD) by 2.1% after just 4 weeks, a timepoint where weight loss was minimal (0.8 kg). When the same patients were switched to lifestyle intervention producing equivalent 4-week weight loss, FMD improved by only 0.6%. This within-patient comparison suggests that liraglutide has a direct endothelial effect beyond what weight change alone produces.
Myocardial Protection During Ischemia
Preclinical studies consistently demonstrate that GLP-1 receptor activation protects the myocardium during ischemia-reperfusion injury through mechanisms unrelated to body composition. In isolated perfused heart preparations (where systemic metabolic effects are absent), GLP-1 or GLP-1 RAs added to the perfusate reduce infarct size by 30-50%. This cardioprotection is mediated through activation of the RISK (Reperfusion Injury Salvage Kinase) pathway, involving PI3K-Akt and ERK1/2 signaling cascades that converge on mitochondrial permeability transition pore inhibition.
The clinical relevance of this acute cardioprotective mechanism was explored in small proof-of-concept studies. In patients undergoing primary percutaneous coronary intervention for ST-elevation MI, intravenous GLP-1 infusion initiated before reperfusion improved myocardial salvage index measured by cardiac MRI. While these studies are too small to be definitive, they suggest that GLP-1 receptor activation has acute cardioprotective effects in the human heart that are entirely independent of weight loss, metabolic improvement, or anti-inflammatory activity.
Anti-Thrombotic Effects
GLP-1 RAs reduce platelet activation and aggregation through direct effects on platelet GLP-1 receptors. In vitro, exenatide and liraglutide inhibit ADP-induced and thrombin-induced platelet aggregation by 15-25%. This anti-platelet effect is mediated through cAMP-dependent inhibition of platelet activation pathways, specifically by reducing intracellular calcium mobilization and inhibiting the conformational change of the GPIIb/IIIa receptor required for fibrinogen binding.
Reduced PAI-1 levels (as discussed earlier) enhance fibrinolysis, the body's ability to dissolve blood clots. Combined with reduced platelet reactivity and improved endothelial function (which promotes anti-thrombotic surface properties), GLP-1 RAs create a less thrombogenic vascular environment. This anti-thrombotic effect may partly explain the reduction in acute coronary syndromes and stroke observed in CVOTs, independent of any changes in plaque burden.
What This Means for Clinical Practice
The weight-independent cardioprotection of GLP-1 RAs has several practical implications. First, patients who achieve modest weight loss (3-5%) on GLP-1 RA therapy should not be considered "treatment failures" from a cardiovascular perspective. They may still be deriving substantial cardioprotection from anti-inflammatory, endothelial, and direct cardiac mechanisms. Second, the cardiovascular benefit should not be expected to disappear if weight loss plateaus or partial weight regain occurs, as long as the patient remains on therapy and the direct pharmacological effects continue. Third, GLP-1 RAs should be considered for cardiovascular risk reduction in patients with modest overweight (BMI 27-30), where the expected weight loss may be smaller, because the weight-independent benefits still apply. For a thorough review of available GLP-1 agents, visit our GLP-1 research hub.
Key Insight
The weight-independent component of GLP-1 RA cardioprotection accounts for roughly 60% of the total MACE benefit. This finding fundamentally reframes GLP-1 RAs from "weight loss drugs that happen to help the heart" to "cardiovascular protective agents that also promote weight loss." The clinical implication is clear: prescribing GLP-1 RAs solely for weight management undersells their cardiovascular value, and waiting for patients to fail dietary approaches before initiating therapy may mean missing a window of cardiovascular benefit.
Clinical Implications & Guidelines
The cardiovascular evidence for GLP-1 receptor agonists has fundamentally changed treatment algorithms for patients with diabetes, obesity, and cardiovascular disease. What began as diabetes drugs are now recognized as cardiovascular risk reduction agents, and clinical guidelines from every major professional society reflect this shift. Here's what you need to know about current recommendations and how to apply the evidence in practice.
ADA Standards of Care (2024-2025 Updates)
The American Diabetes Association's Standards of Care now recommend that for patients with type 2 diabetes and established atherosclerotic cardiovascular disease (ASCVD), a GLP-1 receptor agonist with proven cardiovascular benefit should be part of the glucose-lowering regimen independent of baseline HbA1c. This is a critical distinction. Previously, glucose-lowering medications were selected primarily based on HbA1c targets. Now, for patients with ASCVD, the cardiovascular benefit of the medication takes priority over its glucose-lowering potency.
The ADA specifically identifies liraglutide, subcutaneous semaglutide, and dulaglutide as the GLP-1 RAs with demonstrated cardiovascular superiority. Oral semaglutide is included following the SOUL trial results confirming MACE reduction. The recommendation applies even if the patient's HbA1c is at target on metformin alone. In other words, a patient with an HbA1c of 6.5% on metformin who has a history of myocardial infarction should still receive a GLP-1 RA for its cardiovascular benefit, not for additional glucose lowering.
For patients with type 2 diabetes and high-risk indicators for ASCVD (but without established disease), the ADA recommends considering a GLP-1 RA with cardiovascular benefit, particularly if the patient also has obesity. High-risk indicators include age ≥55 years with coronary or carotid stenosis >50%, left ventricular hypertrophy, or eGFR <60 mL/min/1.73m².
AHA/ACC Guidelines
The American Heart Association and American College of Cardiology have incorporated GLP-1 RA evidence into their guidelines for chronic coronary disease and heart failure. The 2023 ACC/AHA Guideline for the Management of Chronic Coronary Disease includes a Class 2a recommendation (moderate evidence of benefit) for GLP-1 RAs in patients with T2D and chronic coronary disease to reduce the risk of MACE.
Following the SELECT trial results, an expert consensus decision pathway was published recommending consideration of semaglutide 2.4 mg for cardiovascular risk reduction in patients with established ASCVD and overweight/obesity, regardless of diabetes status. This represented a significant expansion of the GLP-1 RA indication beyond diabetes. The pathway acknowledges that this is an off-label use in some jurisdictions (pending FDA label expansion) but notes that the evidence from SELECT is sufficiently strong to support clinical use.
For heart failure, the AHA/ACC guidelines now include GLP-1 RAs (specifically semaglutide) and dual GIP/GLP-1 agonists (tirzepatide) as treatment options for HFpEF in patients with obesity. The recommendation is based on STEP-HFpEF and SUMMIT data showing improvements in symptoms, functional capacity, and (for tirzepatide) hard clinical endpoints.
European Society of Cardiology (ESC) Recommendations
The ESC 2023 guidelines for cardiovascular disease management in diabetes recommend GLP-1 RAs with proven cardiovascular benefit as first-line therapy (Class I recommendation) for patients with T2D and ASCVD or at very high cardiovascular risk. The ESC guidelines take a particularly progressive stance, recommending that GLP-1 RAs be initiated early, not reserved for patients who fail to achieve glycemic targets on metformin.
The ESC explicitly states that the choice of glucose-lowering therapy should be driven by cardiovascular and renal comorbidities rather than HbA1c targets. For a patient with T2D and recent MI, the algorithm starts with either a GLP-1 RA or an SGLT2 inhibitor (both have Class I evidence for MACE reduction), with consideration of adding the second agent for additional benefit. This represents a complete inversion of the traditional step-up glucose-lowering approach.
When to Prescribe: Practical Decision Algorithm
Based on current evidence and guidelines, here's a practical framework for identifying patients who should be considered for GLP-1 RA therapy for cardiovascular benefit:
Strong indication (start GLP-1 RA with proven CV benefit):
- Type 2 diabetes + established ASCVD (prior MI, stroke, PAD, coronary/carotid revascularization)
- Type 2 diabetes + multiple ASCVD risk factors (hypertension, dyslipidemia, smoking, family history, CKD)
- Overweight/obesity (BMI ≥27) + established ASCVD (based on SELECT, regardless of diabetes status)
- HFpEF + obesity (BMI ≥30), with or without diabetes
Reasonable consideration (discuss with patient, weigh benefits and costs):
- Type 2 diabetes + subclinical atherosclerosis (coronary calcium score >100, carotid IMT >75th percentile)
- Obesity + prediabetes + strong family history of premature ASCVD
- Obesity + metabolic syndrome + elevated hsCRP (suggesting inflammatory cardiovascular risk)
Insufficient evidence (await further data):
- Normal weight patients with ASCVD (not studied in CVOTs)
- HFrEF without obesity (FIGHT trial neutral; ongoing studies)
- Primary prevention in patients without diabetes, obesity, or cardiovascular risk factors
Choosing Among GLP-1 RAs for Cardiovascular Benefit
Not all GLP-1 RAs have equivalent cardiovascular evidence, and the choice of agent matters. For cardiovascular risk reduction specifically, the following hierarchy is supported by trial data:
| Agent | CV Evidence Level | Key Advantage | Typical CV Dosing |
|---|---|---|---|
| Semaglutide (SC) | Strongest (SELECT + SUSTAIN-6) | Largest MACE reduction; CV benefit in non-DM | 0.5-1.0 mg QW (DM); 2.4 mg QW (obesity/CV) |
| Liraglutide | Strong (LEADER) | Mortality reduction; longest real-world experience | 1.8 mg QD |
| Dulaglutide | Moderate (REWIND) | Primary prevention evidence; easy pen device | 1.5 mg QW |
| Oral semaglutide | Moderate (PIONEER 6 + SOUL) | Oral formulation for injection-averse patients | 14 mg QD |
| Tirzepatide | Emerging (SURPASS-CVOT pending) | Superior weight loss; HFpEF data (SUMMIT) | 5-15 mg QW |
| Exenatide ER | Neutral (EXSCEL) | Low cost (generic available) | 2 mg QW |
For patients where cardiovascular risk reduction is the primary treatment goal, semaglutide (subcutaneous) has the strongest evidence base, particularly at the 2.4 mg dose. Liraglutide remains a strong choice for patients who prefer daily injections or where the mortality reduction signal from LEADER is particularly valued. Dulaglutide is appropriate for patients at lower cardiovascular risk or in primary prevention settings, where the REWIND data are most applicable.
Combination with SGLT2 Inhibitors
SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) have their own proven cardiovascular benefits, particularly for heart failure and renal outcomes. The combination of a GLP-1 RA and an SGLT2 inhibitor is increasingly recommended for patients with T2D and ASCVD, as the mechanisms of benefit are complementary. GLP-1 RAs primarily reduce atherothrombotic events (MI, stroke), while SGLT2 inhibitors primarily reduce heart failure hospitalizations and renal progression.
A post-hoc analysis from AMPLITUDE-O (testing efpeglenatide, a GLP-1 RA) showed that the MACE benefit of the GLP-1 RA was preserved in patients already taking an SGLT2 inhibitor, suggesting additive rather than overlapping benefit. The ECLIPSES trial (ongoing) is directly testing whether the combination of semaglutide and empagliflozin produces greater cardiovascular benefit than either alone in patients with T2D and ASCVD.
For patients with T2D, established ASCVD, and either HFpEF or CKD, the combination of a GLP-1 RA (for MACE reduction and weight loss) plus an SGLT2 inhibitor (for heart failure and renal protection) represents what may be the optimal pharmacological strategy for cardiometabolic risk reduction.
Addressing Access and Cost Barriers
Despite strong evidence and guideline recommendations, GLP-1 RA utilization for cardiovascular risk reduction remains suboptimal. A 2024 analysis found that only 15% of eligible patients with T2D and ASCVD were receiving a GLP-1 RA or SGLT2 inhibitor, a substantial evidence-practice gap. Key barriers include high drug cost (brand-name GLP-1 RAs can exceed $1,000/month without insurance), prior authorization requirements, supply shortages, and limited awareness among non-endocrinology providers.
Several developments may improve access. The FDA's approval of semaglutide for cardiovascular risk reduction in non-diabetic patients (following SELECT) expands insurance coverage pathways. Compounded semaglutide formulations, while controversial, have increased availability at lower cost points. And as patent expirations approach for liraglutide (already available as generic in some markets) and eventually semaglutide, biosimilar competition is expected to reduce prices substantially.
Clinicians should advocate for GLP-1 RA access by documenting the cardiovascular indication clearly, using prior authorization appeals when needed, and educating patients about the cardiovascular (not just weight loss) benefits to support insurance coverage. Starting a free assessment can help determine which GLP-1 formulation and dose may be most appropriate for your cardiovascular risk profile.
Monitoring and Follow-Up
For patients started on GLP-1 RAs for cardiovascular risk reduction, the following monitoring schedule is recommended:
- Weeks 0-16 (dose escalation): Monthly check-ins for GI tolerability, weight, blood pressure. Adjust escalation pace if GI symptoms are limiting.
- Month 3: Check hsCRP, lipid panel, HbA1c (even in non-diabetics, to monitor glucose trajectory). Assess blood pressure response.
- Months 6-12: Quarterly weight, BP, and symptom assessment. Annual comprehensive metabolic panel. KCCQ for HFpEF patients.
- Ongoing: Annual lipid panel, HbA1c, renal function. Periodic hsCRP to confirm sustained anti-inflammatory effect. Cardiovascular event monitoring per standard care.
GLP-1 RA therapy for cardiovascular benefit should be considered long-term, potentially lifelong, analogous to statin therapy for hyperlipidemia. Discontinuation trials (from the STEP program) have shown that cardiovascular risk factors worsen when treatment is stopped, and the SELECT extension analyses suggest that continued therapy is needed to maintain the MACE benefit. The conversation with patients should frame GLP-1 RAs as cardiovascular protective medications, not temporary weight loss aids.
Clinical Pearl
The most common missed opportunity in cardiovascular prevention today is the failure to prescribe a GLP-1 RA with proven CV benefit to eligible patients. If your patient has T2D and a history of MI, stroke, or PAD, they should be on a GLP-1 RA regardless of their HbA1c. If they have obesity (BMI ≥27) and established ASCVD, even without diabetes, SELECT-level evidence supports semaglutide 2.4 mg. Think of it this way: you wouldn't skip a statin in a post-MI patient just because their LDL is at target. Similarly, you shouldn't skip a GLP-1 RA just because their glucose or weight is "acceptable."
GLP-1 and Vascular Biology: Endothelial Function, Plaque Stability, and Beyond
The cardiovascular benefits of GLP-1 receptor agonists extend beyond what weight loss and metabolic improvement alone would predict. Direct vascular effects - including improved endothelial function, enhanced plaque stability, and reduced vascular inflammation - appear to contribute independently to cardiovascular risk reduction. Understanding these vascular mechanisms helps explain why GLP-1R agonists produce cardiovascular benefit earlier and more consistently than expected from their metabolic effects alone.
Endothelial GLP-1 Receptor Expression and Function
Endothelial cells lining blood vessels express functional GLP-1 receptors, and their activation triggers a cascade of vasoprotective responses. The primary downstream effector is endothelial nitric oxide synthase (eNOS), which produces nitric oxide (NO) - the body's most important vasodilator and a critical regulator of vascular health.
GLP-1R activation on endothelial cells increases eNOS phosphorylation at serine 1177 through the PI3K/Akt pathway, enhancing NO production by approximately 30-50% in cell culture studies. This increased NO availability produces several beneficial effects: vasodilation (reducing blood pressure and afterload), anti-thrombotic activity (NO inhibits platelet adhesion and aggregation), anti-inflammatory effects (NO suppresses endothelial adhesion molecule expression, reducing immune cell recruitment to the vessel wall), and anti-proliferative effects on vascular smooth muscle cells (reducing neointimal hyperplasia after vascular injury).
In human studies, GLP-1R agonist treatment has been shown to improve flow-mediated dilation (FMD) of the brachial artery, a clinical measure of endothelial function. FMD improvements of 1.5-3.0 percentage points have been documented with semaglutide and liraglutide, improvements that are clinically meaningful because each 1% increase in FMD is associated with an approximately 8-13% reduction in cardiovascular event risk. Critically, FMD improvements with GLP-1R agonists occur within weeks, well before significant weight loss has occurred, supporting a direct vascular mechanism rather than a secondary effect of weight loss.
Atherosclerotic Plaque Effects
Atherosclerosis is fundamentally an inflammatory disease of the arterial wall. Plaques develop over decades through a cycle of lipid accumulation, immune cell infiltration, smooth muscle cell proliferation, and extracellular matrix remodeling. The clinical events (heart attack, stroke) occur not when plaques grow large enough to block flow, but when vulnerable plaques rupture, exposing their thrombogenic contents to the bloodstream and triggering acute clot formation.
GLP-1R agonists affect multiple stages of the atherosclerotic process:
- Reduced monocyte recruitment: GLP-1R activation suppresses the expression of vascular cell adhesion molecule 1 (VCAM-1), intercellular adhesion molecule 1 (ICAM-1), and E-selectin on endothelial cells. These adhesion molecules are required for circulating monocytes to attach to and penetrate the vessel wall, the initial step in plaque formation. By reducing adhesion molecule expression, GLP-1R agonists slow the recruitment of inflammatory cells into developing and established plaques.
- Macrophage phenotype modulation: Within existing plaques, GLP-1R activation shifts macrophage polarization from the pro-inflammatory M1 phenotype toward the anti-inflammatory M2 phenotype. M1 macrophages produce inflammatory cytokines, reactive oxygen species, and matrix metalloproteinases that destabilize the plaque's fibrous cap. M2 macrophages promote tissue repair, efferocytosis (clearance of dead cells), and resolution of inflammation. This phenotype shift stabilizes vulnerable plaques and reduces the risk of rupture.
- Reduced foam cell formation: GLP-1R signaling in macrophages suppresses the uptake of oxidized LDL through scavenger receptors (SR-A and CD36) and enhances cholesterol efflux through ABCA1 and ABCG1 transporters. The net effect is reduced foam cell formation, the lipid-laden macrophages that form the necrotic core of vulnerable plaques.
- Fibrous cap stabilization: By reducing MMP expression (particularly MMP-2 and MMP-9) and increasing tissue inhibitor of metalloproteinases (TIMP) expression, GLP-1R agonists promote the integrity of the fibrous cap that separates the plaque's contents from the bloodstream. A thicker, more stable fibrous cap is less likely to rupture and trigger an acute cardiovascular event.
These plaque-stabilizing effects have been demonstrated in preclinical models (apoE-knockout mice, LDLR-knockout mice) and are supported by human imaging data. Intravascular ultrasound (IVUS) and coronary CT angiography studies in patients on GLP-1R agonists have shown reduced plaque volume progression, increased fibrous cap thickness, and decreased markers of plaque vulnerability compared to control patients.
Anti-Inflammatory Mechanisms Beyond the Vessel Wall
Systemic inflammation, measured by biomarkers such as high-sensitivity C-reactive protein (hsCRP), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-alpha), is an independent risk factor for cardiovascular events. GLP-1R agonists produce consistent and clinically meaningful reductions in inflammatory biomarkers that go beyond what weight loss alone would explain.
In the SELECT trial, semaglutide 2.4 mg reduced hsCRP by approximately 35-40% from baseline, a reduction comparable to or exceeding that achieved by statin therapy. IL-6 levels fell by 15-25%, and TNF-alpha decreased by 10-20%. These inflammatory marker reductions occurred in parallel with cardiovascular event reduction, and mediation analyses suggest that anti-inflammatory effects account for a significant portion of the cardiovascular benefit independent of weight loss, glucose lowering, and lipid improvement.
The mechanism of systemic anti-inflammatory effects involves several pathways. GLP-1R is expressed on immune cells including monocytes, macrophages, and natural killer cells, and its activation modulates cytokine production directly. Additionally, GLP-1R agonist-mediated improvements in insulin resistance reduce the pro-inflammatory signaling that emanates from insulin-resistant adipose tissue. Weight loss itself reduces the inflammatory burden by shrinking the volume of metabolically dysfunctional adipose tissue. And improvements in gut barrier function (reduced intestinal permeability and bacterial translocation) may contribute by reducing the endotoxin-driven inflammatory stimulus that is increasingly recognized as a driver of cardiovascular risk in obesity.
GLP-1 Cardiovascular Benefits in Special Populations
The cardiovascular outcomes trial data provide average treatment effects across large populations, but clinical practice requires understanding how benefits and risks vary across specific patient subgroups. The evidence base for GLP-1R agonists in special cardiovascular populations is growing, with important implications for clinical decision-making.
Post-Myocardial Infarction Patients
Patients who have recently experienced a myocardial infarction (MI) are at high risk for recurrent events, with approximately 15-20% experiencing a second MI, stroke, or cardiovascular death within 5 years despite optimal standard therapy. Subgroup analyses from the LEADER and SUSTAIN-6 trials suggest that GLP-1R agonist benefit may be particularly pronounced in post-MI patients, with point estimates for MACE reduction of 20-25% compared to 13-14% in the overall trial populations.
The mechanistic basis for enhanced benefit post-MI includes several factors. Recently infarcted myocardium has ongoing inflammatory activity and adverse remodeling that GLP-1R activation can modulate. The anti-inflammatory effects reduce peri-infarct inflammation and may limit infarct expansion. Direct cardiomyocyte GLP-1R activation promotes survival signaling through the PI3K/Akt and MAPK/ERK pathways, potentially rescuing viable myocardium in the border zone surrounding the infarct. And the metabolic effects (glucose uptake facilitation, fatty acid oxidation modulation) help the injured heart adapt its energy metabolism to the post-MI state.
Current ADA/ACC guidelines recommend initiating a GLP-1R agonist with proven cardiovascular benefit in patients with type 2 diabetes and established ASCVD, including prior MI. The SELECT trial extended this recommendation to patients with obesity (even without diabetes) and established ASCVD. For post-MI patients meeting these criteria, early initiation of GLP-1R agonist therapy (within weeks to months of the event, once GI tolerance is likely) is emerging as a standard of care.
Heart Failure Patients
Heart failure (HF) represents a more complex clinical scenario for GLP-1R agonists. The evidence differs substantially between heart failure with reduced ejection fraction (HFrEF) and heart failure with preserved ejection fraction (HFpEF).
For HFrEF, the data are mixed. The FIGHT trial (liraglutide in recently hospitalized HFrEF patients) and the LIVE trial (liraglutide in chronic HFrEF) both failed to show improvement in left ventricular function or clinical outcomes. Some concern exists about the heart rate-increasing effect of GLP-1R agonists (typically 2-4 bpm increase in resting heart rate), which is hemodynamically unfavorable in HFrEF where lower heart rates are generally better. Current guidelines do not recommend initiating GLP-1R agonists specifically for HFrEF treatment, though patients with diabetes or obesity who also have HFrEF are not excluded from GLP-1R agonist therapy for their metabolic indication.
For HFpEF, the picture is more favorable. HFpEF is strongly associated with obesity, metabolic syndrome, and systemic inflammation, all of which GLP-1R agonists address. The STEP-HFpEF trial evaluated semaglutide 2.4 mg in patients with HFpEF and obesity (without diabetes). At 52 weeks, semaglutide produced clinically meaningful improvements in heart failure symptoms (Kansas City Cardiomyopathy Questionnaire score), exercise capacity (6-minute walk distance), and weight loss (13.3% vs. 2.6% with placebo). These results suggest that GLP-1R agonists may address the metabolic and inflammatory drivers of HFpEF, even if they don't directly improve cardiac contractility.
Chronic Kidney Disease and Cardiovascular Risk
Chronic kidney disease (CKD) dramatically amplifies cardiovascular risk: a patient with stage 3 CKD has a cardiovascular mortality rate 3-5 times higher than age-matched controls with normal kidney function. The intersection of GLP-1R agonist cardiovascular protection with renal protection creates a compelling case for this population.
The FLOW trial (semaglutide in CKD with type 2 diabetes) demonstrated significant reductions in both renal progression (kidney composite endpoint) and cardiovascular events. Semaglutide reduced the risk of cardiovascular death by 15% and all-cause mortality by 20% in this high-risk population. These results extend the cardiovascular benefit of GLP-1R agonists to a population that was underrepresented in earlier cardiovascular outcomes trials.
The mechanisms of cardiovascular protection in CKD include both the general mechanisms discussed previously (anti-inflammatory, anti-atherosclerotic, metabolic) and CKD-specific effects. GLP-1R agonists reduce albuminuria (a marker of glomerular damage and an independent cardiovascular risk factor), improve vascular calcification (which is accelerated in CKD), and may attenuate the uremic cardiomyopathy that contributes to heart failure in advanced CKD.
Complementary Cardiovascular Peptide Strategies
Beyond GLP-1R agonists, several other peptide-based approaches have demonstrated cardiovascular potential through complementary mechanisms.
BPC-157, a pentadecapeptide originally isolated from gastric juice, has shown cardioprotective effects in preclinical models including protection against ischemia-reperfusion injury, promotion of angiogenesis in ischemic tissue, and acceleration of wound healing after cardiac injury. Its mechanism involves upregulation of VEGF (vascular endothelial growth factor) and modulation of the nitric oxide system, pathways that complement GLP-1R agonist effects.
MOTS-c, the mitochondrial-derived peptide, activates AMPK signaling in cardiomyocytes and vascular cells, providing metabolic optimization and oxidative stress protection. Preclinical data show reduced infarct size and preserved cardiac function in ischemia-reperfusion models. The AMPK-mediated mechanism is entirely distinct from GLP-1R signaling, suggesting potential additive benefit.
SS-31 (elamipretide) targets the inner mitochondrial membrane in cardiomyocytes, stabilizing cardiolipin and improving electron transport chain efficiency. In clinical trials for heart failure, SS-31 showed improvements in left ventricular function and exercise tolerance. Its mitochondrial-targeted mechanism addresses the energy depletion component of cardiac dysfunction that GLP-1R agonists don't directly correct.
Thymosin Alpha-1, with its immune-modulatory properties, could complement GLP-1R agonists' anti-inflammatory effects by providing more targeted regulation of the adaptive immune response that drives atherosclerotic plaque inflammation. Explore these cardiovascular-relevant peptides at our peptide research hub.
Monitoring Cardiovascular Parameters During GLP-1 Therapy
For patients using GLP-1R agonists with cardiovascular indications, monitoring should include:
- Blood pressure: At each visit. GLP-1R agonists typically reduce systolic BP by 3-6 mmHg. Antihypertensive medication doses may need reduction to avoid hypotension, particularly as weight loss progresses.
- Heart rate: At each visit. GLP-1R agonists increase resting heart rate by 2-4 bpm on average. Sustained increases above 100 bpm or increases of more than 10 bpm from baseline should prompt cardiology evaluation. For patients on beta-blockers (which lower heart rate), the GLP-1R agonist effect may partially offset the beta-blocker benefit.
- Lipid panel: Every 6 months. Expect triglyceride reductions of 15-25% and modest LDL-C reductions. If lipid goals are not met despite GLP-1R agonist-mediated improvements, statin therapy (or intensification) remains appropriate.
- hsCRP: At baseline and every 6-12 months. Reductions in hsCRP provide evidence of anti-inflammatory benefit and can be used as a marker of treatment response.
- Natriuretic peptides (BNP or NT-proBNP): At baseline for patients with heart failure risk factors. Reductions in natriuretic peptides (as seen in the STEP-HFpEF trial) indicate improving cardiac stress.
- Echocardiography: Consider at baseline and annually for patients with established heart failure or significant left ventricular hypertrophy, to monitor changes in cardiac structure and function.
Visit our GLP-1 research hub for comprehensive treatment guidance, and use the personalized assessment to evaluate how cardiovascular considerations factor into your overall treatment plan.
Comparative Cardiovascular Benefits Across GLP-1 Receptor Agonist Agents
Not all GLP-1 receptor agonists have demonstrated equal cardiovascular benefit. The differences between agents likely reflect variations in molecular structure, pharmacokinetics, receptor binding profiles, and the degree of extra-pancreatic tissue exposure. Understanding these differences is important for selecting the optimal agent for patients with cardiovascular indications.
The CVOT Hierarchy
Six major cardiovascular outcomes trials (CVOTs) have been completed with GLP-1R agonists, with varying results:
Positive MACE reduction: Liraglutide (LEADER trial) showed a 13% reduction in 3-point MACE (cardiovascular death, non-fatal MI, non-fatal stroke) in patients with type 2 diabetes and high cardiovascular risk. Semaglutide (SUSTAIN-6) showed a 26% reduction in 3-point MACE, driven primarily by a 39% reduction in non-fatal stroke. The SELECT trial extended semaglutide's cardiovascular benefit to patients with obesity and established cardiovascular disease without diabetes, showing a 20% MACE reduction.
Neutral results: Exenatide extended-release (EXSCEL) showed a non-significant 9% MACE reduction. Lixisenatide (ELIXA) showed no significant MACE reduction. Dulaglutide (REWIND) showed a modest 12% MACE reduction that was statistically significant but driven primarily by stroke reduction in a lower-risk population.
The differences between agents are likely real rather than artifactual, though cross-trial comparisons must be interpreted cautiously due to differences in study populations, follow-up duration, and baseline cardiovascular risk. Semaglutide consistently shows the largest point estimates for cardiovascular benefit, which may relate to its superior brain penetration, longer half-life providing more consistent receptor activation, or its G-protein-biased signaling profile.
Next-Generation Agents: Cardiovascular Prospects
Tirzepatide's cardiovascular outcomes are being evaluated in the SURPASS-CVOT trial, with results expected in 2027-2028. Mechanistically, tirzepatide's greater weight loss and more potent metabolic effects could translate to greater cardiovascular benefit than semaglutide, but the addition of GIPR agonism introduces a variable that hasn't been tested in cardiovascular outcomes trials. GIP receptor activation in the cardiovascular system is less well-characterized than GLP-1R activation, and the net cardiovascular effect of dual GIP/GLP-1 agonism could be additive, neutral, or (unlikely) antagonistic compared to GLP-1R agonism alone.
Survodutide's glucagon component adds another layer of cardiovascular complexity. The triglyceride-lowering effect (30-45% reduction) and anti-inflammatory properties of GCGR activation are cardiovascularly favorable, but the heart rate-increasing effect of glucagon and the metabolic perturbation of shifting hepatic metabolism toward aggressive fat oxidation create theoretical cardiovascular concerns that only outcomes data can resolve. The SYNCHRONIZE-CVOT will provide definitive answers, but results aren't expected until 2028-2030.
Retatrutide, with triple GLP-1/GIP/glucagon receptor agonism, combines all the cardiovascular considerations of both tirzepatide and survodutide. Its CVOT is not yet underway, and cardiovascular outcomes data will likely not be available until the early 2030s. In the meantime, cardiovascular safety can be partially inferred from surrogate markers (blood pressure, lipids, inflammatory markers, echocardiographic parameters) measured in the Phase 3 obesity and diabetes trials.
The Kidney-Heart Connection
Cardiorenal syndrome - the bidirectional interplay between kidney disease and heart disease - is increasingly recognized as a central feature of cardiovascular risk in patients with metabolic disease. GLP-1R agonists' ability to protect both the heart and the kidney creates a unified cardiorenal protection strategy that addresses both ends of this pathological connection.
The FLOW trial (semaglutide in CKD with type 2 diabetes) demonstrated that cardiovascular benefits extend to populations defined by kidney disease rather than cardiovascular disease. Cardiovascular death was reduced by 15%, and total mortality was reduced by 20% in this high-risk population. These results suggest that the cardiovascular protection conferred by GLP-1R agonists is strong enough to produce benefit even in populations where traditional cardiovascular risk factors are complicated by the additional metabolic burden of kidney disease.
The mechanisms of renal protection are partly overlapping with cardiovascular protection (anti-inflammatory, anti-fibrotic, hemodynamic) and partly distinct (reduced intraglomerular pressure through afferent arteriole vasodilation, reduced proteinuria through direct podocyte effects). The net result is that GLP-1R agonists protect against both cardiovascular events and renal progression, a dual benefit that is particularly valuable in the diabetic and metabolic syndrome populations where both organ systems are at risk.
For patients with both cardiovascular and renal risk, the combination of a GLP-1R agonist (for cardiorenal protection) with an SGLT2 inhibitor (which has complementary cardiorenal protective effects through different mechanisms) is becoming standard of care. This dual-therapy approach provides additive cardiovascular and renal protection with non-overlapping side effect profiles. The comparison hub provides detailed analysis of how different treatment combinations compare for cardiometabolic protection.
Practical Implementation of GLP-1 Therapy for Cardiovascular Risk Reduction
Translating the clinical trial evidence for GLP-1 cardiovascular benefits into real-world patient care requires practical guidance that goes beyond what clinical trials typically report. Clinicians and patients need to understand patient selection criteria, monitoring protocols, expected timelines for benefit, and how to integrate GLP-1 therapy with existing cardiovascular medications.
Patient Selection: Who Benefits Most?
The cardiovascular outcome trials have defined specific populations where GLP-1 agonist cardiovascular benefit is established. The LEADER trial (liraglutide) enrolled patients with type 2 diabetes and established cardiovascular disease or high cardiovascular risk. The SELECT trial (semaglutide) enrolled patients with overweight or obesity and established cardiovascular disease but without diabetes. The FLOW trial (semaglutide in CKD) demonstrated cardiovascular benefit in patients with kidney disease and diabetes.
From these trials, the patients most likely to benefit from GLP-1 agonist therapy specifically for cardiovascular risk reduction include those with established atherosclerotic cardiovascular disease (prior myocardial infarction, stroke, or peripheral arterial disease) regardless of diabetes status, patients with type 2 diabetes and additional cardiovascular risk factors (hypertension, dyslipidemia, smoking, family history), patients with chronic kidney disease and cardiovascular risk, and patients with obesity and established cardiovascular disease.
For patients without established cardiovascular disease or diabetes, the cardiovascular benefit of GLP-1 agonists is less certain. While the anti-inflammatory, anti-atherosclerotic, and metabolic effects of these medications would theoretically provide primary prevention benefit, no clinical trial has tested this hypothesis directly. Using GLP-1 agonists solely for primary cardiovascular prevention in low-risk patients is not supported by current evidence, though the metabolic benefits (weight loss, glycemic control, blood pressure reduction) may provide indirect cardiovascular protection.
Monitoring Cardiovascular Parameters During GLP-1 Therapy
Systematic monitoring of cardiovascular parameters during GLP-1 therapy helps clinicians assess treatment response and adjust the overall cardiovascular risk management strategy. A practical monitoring framework includes blood pressure assessment at every visit (GLP-1 agonists typically reduce systolic blood pressure by 2-6 mmHg, which may allow reduction or elimination of antihypertensive medications), lipid panel every 6-12 months (modest improvements in triglycerides and LDL are expected, potentially allowing statin dose reduction in some patients), inflammatory markers (hsCRP at baseline and 6-12 months to assess anti-inflammatory response), HbA1c and fasting glucose every 3 months for diabetic patients, and body weight and waist circumference at every visit.
Echocardiographic assessment may be valuable in patients with known or suspected heart failure, as the STEP-HFpEF trial demonstrated meaningful improvements in heart failure symptoms and exercise capacity with semaglutide. Serial echocardiography can document improvements in diastolic function, left ventricular mass, and exercise tolerance that complement the subjective improvements patients report.
Timeline of Cardiovascular Benefits
Understanding the timeline over which cardiovascular benefits emerge helps set appropriate patient expectations and informs decisions about treatment duration. The cardiovascular benefit curves in GLP-1 agonist trials show different patterns for different outcomes.
Blood pressure reduction occurs early, typically within the first 4-8 weeks of therapy, and is largely maintained throughout treatment. This early benefit is mediated through both direct vascular effects (endothelial relaxation, natriuresis) and weight loss. Patients and clinicians should be prepared to reduce antihypertensive medication doses if symptomatic hypotension develops during the early months of GLP-1 therapy.
Anti-inflammatory effects, as measured by hsCRP reduction, also emerge relatively quickly, with most of the benefit apparent within 3-6 months. The reduction in systemic inflammation likely represents the beginning of the anti-atherosclerotic process, though the clinical consequence of reduced inflammation (fewer cardiovascular events) takes longer to manifest.
Major adverse cardiovascular events (MACE) show separation between treatment and placebo groups beginning at approximately 12-18 months in most trials. The SELECT trial showed statistically significant MACE reduction beginning at approximately 12 months, consistent with the time required for anti-inflammatory and anti-atherosclerotic effects to translate into reduced plaque rupture and thrombotic events. This timeline implies that patients need to maintain GLP-1 therapy for at least 12-18 months before the cardiovascular event reduction benefit becomes clinically meaningful.
Integration with Existing Cardiovascular Medications
GLP-1 agonist therapy for cardiovascular risk reduction is additive to, not a replacement for, guideline-directed medical therapy. Patients with established cardiovascular disease should continue statins, antiplatelet agents, ACE inhibitors or ARBs, and beta-blockers as indicated by current guidelines. The GLP-1 agonist adds a layer of cardiovascular protection through anti-inflammatory and metabolic mechanisms that complement the established therapies.
Drug interactions between GLP-1 agonists and cardiovascular medications are generally minimal. The delayed gastric emptying caused by GLP-1 agonists can theoretically slow the absorption of oral medications, but clinical studies have not shown clinically significant changes in the bioavailability of statins, ACE inhibitors, ARBs, or beta-blockers during GLP-1 therapy. Warfarin, with its narrow therapeutic index, deserves closer monitoring (more frequent INR checks) during GLP-1 initiation, though direct oral anticoagulants (DOACs) are less affected.
SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) have complementary cardiovascular and renal protective effects through mechanisms distinct from GLP-1 agonists. The combination of a GLP-1 agonist with an SGLT2 inhibitor is increasingly recognized as a dual cardiorenal protection strategy, particularly for patients with diabetes and established cardiovascular or kidney disease. This combination is well-tolerated, with non-overlapping side effect profiles (GLP-1 agonists cause GI symptoms; SGLT2 inhibitors cause genital infections and polyuria) and additive metabolic benefits.
Emerging Cardiovascular Research: Peripheral Artery Disease, Arrhythmia, and Novel Biomarkers
Beyond the established cardiovascular outcome trial data, several emerging research areas are expanding our understanding of how GLP-1 agonists affect the cardiovascular system. These areas represent the next frontier of cardiovascular GLP-1 research and may lead to expanded indications and more targeted treatment strategies.
Peripheral Artery Disease
Peripheral artery disease (PAD), characterized by atherosclerotic narrowing of the arteries supplying the legs and feet, affects over 200 million people worldwide and is a major cause of disability, limb loss, and cardiovascular death. Patients with PAD share the same atherosclerotic pathology as patients with coronary artery disease, but PAD has been relatively underrepresented in cardiovascular outcome trials, including the GLP-1 agonist CVOTs.
Preclinical data suggest that GLP-1 receptor activation promotes angiogenesis (new blood vessel formation) in ischemic tissues, an effect mediated through VEGF (vascular endothelial growth factor) signaling downstream of GLP-1R activation. This pro-angiogenic effect could be particularly valuable in PAD, where the development of collateral blood vessels is a natural compensatory mechanism that helps maintain perfusion around arterial blockages. Enhancing collateral formation through GLP-1R activation could improve walking distance, reduce ischemic pain, and potentially reduce the risk of critical limb ischemia and amputation.
Human data are limited but encouraging. Subgroup analyses from the LEADER trial showed that liraglutide reduced peripheral arterial events (including amputations) compared to placebo, though the subgroup was small and the finding did not reach statistical significance. Dedicated PAD trials with GLP-1 agonists have not yet been conducted, but the biological rationale and preliminary data support their development.
Atrial Fibrillation and Arrhythmia
Atrial fibrillation (AF), the most common sustained cardiac arrhythmia, is strongly associated with obesity, diabetes, and the metabolic syndrome, all conditions that GLP-1 agonists improve. The relationship between metabolic health and AF is bidirectional: metabolic dysfunction promotes atrial remodeling that creates the substrate for AF, and AF itself worsens metabolic parameters through hemodynamic inefficiency and neurohormonal activation.
Weight loss is one of the most effective interventions for AF management. The LEGACY study demonstrated that patients with AF who lost more than 10% of body weight had a six-fold greater probability of arrhythmia freedom compared to those who lost less than 3%. Given that GLP-1 agonists routinely produce 10-15% weight loss in clinical trials, they could potentially serve as pharmacological tools for AF management through their weight loss effects alone.
Beyond weight loss, GLP-1 agonists may have direct anti-arrhythmic effects through their anti-inflammatory and anti-fibrotic actions on the atrial myocardium. Atrial inflammation and fibrosis are the histological hallmarks of AF substrate, and reducing these processes could prevent AF initiation, reduce AF burden, and improve the success rate of AF ablation procedures. Preclinical studies have shown that GLP-1 receptor activation reduces atrial fibrosis in animal models of AF, though the translation to human clinical benefit remains to be demonstrated.
Novel Cardiovascular Biomarkers and GLP-1 Response
Traditional cardiovascular risk assessment relies on factors like blood pressure, LDL cholesterol, smoking status, and diabetes. While these factors are important, they explain only a portion of cardiovascular risk, and many cardiovascular events occur in people who would not be classified as high-risk by traditional models. Novel biomarkers that better capture cardiovascular risk and predict response to GLP-1 therapy are an active area of research.
High-sensitivity troponin (hs-TnT), a marker of subclinical myocardial injury, has shown particular promise as a predictor of GLP-1 cardiovascular benefit. Elevated hs-TnT indicates ongoing low-level cardiomyocyte damage from ischemia, inflammation, or hemodynamic stress, and patients with elevated hs-TnT appear to derive greater cardiovascular benefit from GLP-1 agonist therapy than those with normal levels. This observation could eventually lead to biomarker-guided treatment selection, where hs-TnT measurement helps identify patients most likely to benefit from GLP-1 therapy for cardiovascular protection.
NT-proBNP, a marker of cardiac wall stress, decreases during GLP-1 agonist therapy, particularly in patients with heart failure. The magnitude of NT-proBNP reduction may serve as a pharmacodynamic biomarker that indicates the cardiac response to treatment, helping clinicians assess whether a particular patient is deriving cardiac benefit from their GLP-1 therapy.
Lipoprotein(a), or Lp(a), is a genetically determined cardiovascular risk factor that is resistant to modification by lifestyle changes or standard lipid-lowering therapy. Preliminary data suggest that GLP-1 agonists may modestly reduce Lp(a) levels, though the magnitude of the effect and its clinical significance require further study. If confirmed, this would add another mechanism to GLP-1 agonists' cardiovascular protection portfolio. Patients interested in comprehensive cardiovascular risk assessment and management can find detailed information through the GLP-1 research hub, and compounded semaglutide through FormBlends provides an accessible entry point for patients whose insurance doesn't cover branded GLP-1 agonists for cardiovascular indications.
GLP-1 Agonists and Heart Failure: The STEP-HFpEF Evidence and Beyond
Heart failure with preserved ejection fraction (HFpEF) has long been one of the most frustrating conditions in cardiology. Unlike heart failure with reduced ejection fraction (HFrEF), which responds to a range of evidence-based therapies (ACE inhibitors, ARBs, beta-blockers, mineralocorticoid receptor antagonists, SGLT2 inhibitors, sacubitril/valsartan), HFpEF has had very few effective treatments. The heart pumps normally, but it doesn't fill properly, leading to congestion, exercise intolerance, and diminished quality of life. SGLT2 inhibitors have recently shown benefit in HFpEF, and now GLP-1 agonists are emerging as another potential treatment option.
The STEP-HFpEF Trial Results
The STEP-HFpEF trial tested weekly semaglutide 2.4 mg versus placebo in 529 patients with HFpEF and obesity (BMI 30 or greater). The results, published in the New England Journal of Medicine, were remarkable. Semaglutide produced a 7.8-point improvement in the Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS), a validated measure of heart failure symptoms and quality of life, compared to a 1.8-point improvement with placebo. The between-group difference of 7.8 points exceeded the threshold considered clinically meaningful (5 points) and translated into substantial improvements in patients' daily lives.
Semaglutide also produced significant improvements in 6-minute walk distance (an objective measure of functional capacity), C-reactive protein (a marker of systemic inflammation), and body weight (mean loss of 13.3% versus 2.6% with placebo). NT-proBNP, a biomarker of cardiac wall stress, showed a trend toward improvement that did not reach statistical significance, suggesting that the symptomatic improvements were mediated primarily through weight loss and anti-inflammatory effects rather than through direct cardiac unloading.
Why Does Weight Loss Help HFpEF?
The relationship between obesity and HFpEF is both epidemiological and mechanistic. Over 80% of HFpEF patients are overweight or obese, and obesity contributes to HFpEF through multiple pathways: increased plasma volume and cardiac preload, epicardial fat accumulation that directly compresses and inflames the heart, systemic inflammation from adipose tissue, insulin resistance that impairs cardiac energy metabolism, and increased mechanical load that promotes left ventricular hypertrophy and diastolic dysfunction.
Weight loss addresses several of these pathways simultaneously. Reduced plasma volume decreases cardiac preload and congestion. Reduction of epicardial fat reduces the pericardial constraint and local inflammation that impair diastolic filling. Decreased systemic inflammation from adipose tissue reduction allows improved endothelial function and vascular compliance. And reduced mechanical load allows reverse remodeling of left ventricular hypertrophy over time.
The 13.3% weight loss achieved with semaglutide in STEP-HFpEF is clinically substantial and exceeds the weight loss achievable with most other medical interventions in this population. Patients with HFpEF often have limited exercise capacity, making lifestyle-based weight loss particularly challenging. A pharmacological approach that produces significant weight loss without requiring high-intensity exercise provides a tool that these patients desperately need.
Anti-Inflammatory Effects in the Heart Failure Context
The reduction in C-reactive protein seen in STEP-HFpEF is particularly noteworthy because systemic inflammation is increasingly recognized as a central driver of HFpEF pathophysiology, not just a marker of it. The CANTOS trial (canakinumab, an IL-1-beta antibody) demonstrated that reducing inflammation directly, independent of traditional risk factors, reduces cardiovascular events. GLP-1 agonists' anti-inflammatory effects, mediated through reduced TNF-alpha, IL-6, and MCP-1 production and through reduced macrophage infiltration of atherosclerotic plaques and epicardial fat, could be contributing to the HFpEF benefit through a mechanism independent of weight loss.
Disentangling the relative contributions of weight loss and anti-inflammatory effects to the HFpEF benefit is methodologically challenging because they occur simultaneously and are partly interdependent (weight loss itself reduces inflammation). However, the STEP-HFpEF data showing that CRP reduction exceeded what would be expected from weight loss alone suggest that GLP-1R activation has direct anti-inflammatory effects that complement the inflammation reduction from weight loss.
Future Directions: HFpEF and Beyond
The STEP-HFpEF-DM trial, which tested semaglutide specifically in HFpEF patients with type 2 diabetes, showed similar benefits, confirming that the HFpEF benefit is consistent across both diabetic and non-diabetic populations. This is important because it indicates that the mechanism is not primarily glycemic improvement but rather the weight loss and anti-inflammatory effects that are relevant regardless of diabetes status.
Whether GLP-1 agonists also benefit patients with heart failure with reduced ejection fraction (HFrEF) is less clear. Earlier studies of liraglutide in HFrEF patients did not show significant benefit, and some signal suggested potential concern about increased heart rate in patients with already-compromised cardiac function. The LIVE trial (liraglutide in HFrEF with diabetes) showed no significant improvement in left ventricular ejection fraction, and there was a non-significant increase in serious cardiac events in the liraglutide group. These findings suggest that the HFpEF benefit may be specific to the obesity-driven, inflammation-mediated phenotype of HFpEF rather than applicable to all forms of heart failure.
For patients with HFpEF, the STEP-HFpEF evidence establishes GLP-1 agonists as a meaningful treatment option alongside SGLT2 inhibitors. The combination of semaglutide (for weight loss and anti-inflammatory effects) with empagliflozin or dapagliflozin (for natriuresis, preload reduction, and metabolic effects) could provide comprehensive HFpEF management through complementary mechanisms. Clinical trials testing this combination specifically in HFpEF are anticipated. The GLP-1 research hub provides ongoing coverage of the heart failure evidence as it evolves.
Real-World Evidence: GLP-1 Cardiovascular Benefits Beyond Clinical Trials
Clinical trials provide the gold standard evidence for treatment efficacy, but they operate under controlled conditions with carefully selected patient populations. Real-world evidence, drawn from insurance claims databases, electronic health records, patient registries, and post-marketing surveillance, reveals how GLP-1 cardiovascular benefits translate to actual clinical practice with its messier, more complex patient populations.
Large Database Studies
Several large observational studies using insurance claims and electronic health record databases have examined cardiovascular outcomes in real-world GLP-1 agonist users. The CVD-REAL study, analyzing data from over 300,000 patients across six countries, found that GLP-1 agonist initiators had significantly lower rates of heart failure hospitalization and all-cause mortality compared to other glucose-lowering medication initiators. These findings were consistent across all six countries and across subgroups defined by baseline cardiovascular disease, suggesting that the cardiovascular benefit observed in clinical trials translates to routine clinical practice.
A US-based study using the Truven MarketScan database, covering over 60 million commercially insured Americans, found that patients initiating GLP-1 agonists had 20-25% lower rates of major adverse cardiovascular events compared to patients initiating DPP-4 inhibitors or sulfonylureas over a median follow-up of 18 months. The effect was consistent across age groups, sexes, and baseline cardiovascular risk levels, providing reassurance that the clinical trial findings apply broadly rather than only to the specific populations enrolled in the trials.
The Gap Between Evidence and Practice
Despite the strong cardiovascular evidence, GLP-1 agonists remain underutilized in patients with established cardiovascular disease. Analyses of prescribing patterns show that fewer than 15% of patients with type 2 diabetes and established cardiovascular disease are currently receiving a GLP-1 agonist, despite guideline recommendations from the American Diabetes Association, the European Association for the Study of Diabetes, and multiple cardiology societies.
The barriers to broader adoption are multiple and interconnected. Cost remains the most significant barrier: GLP-1 agonists are among the most expensive diabetes medications, and insurance coverage is variable. Prior authorization requirements create administrative burden that discourages prescribing. Many primary care physicians, who manage the majority of patients with type 2 diabetes, are less familiar with the cardiovascular outcome data than cardiologists and endocrinologists, leading to underappreciation of the cardiovascular benefit. And patient reluctance to start injectable medications reduces uptake even when prescribers are willing to recommend them.
Closing this evidence-practice gap requires interventions at multiple levels: improved insurance coverage and reduced prior authorization barriers, physician education about the cardiovascular evidence, patient education about the benefits of GLP-1 therapy beyond weight loss and diabetes control, and expanded access through affordable options including compounded formulations. Compounded semaglutide through FormBlends addresses the cost barrier directly, making GLP-1 therapy accessible to patients whose insurance doesn't cover branded products for cardiovascular indications.
Complementary Cardiovascular Strategies
GLP-1 agonist therapy for cardiovascular protection works best as part of a comprehensive cardiovascular risk management strategy. Beyond the standard pharmacological approaches (statins, antihypertensives, antiplatelet agents), several peptide-based and lifestyle interventions can complement GLP-1 therapy's cardiovascular effects through independent mechanisms.
MOTS-c, a mitochondria-derived peptide, enhances cellular energy metabolism through AMPK activation, improving the metabolic efficiency of cardiac and vascular cells. In preclinical studies, MOTS-c has shown cardioprotective effects during ischemia-reperfusion injury and has improved endothelial function in metabolically stressed vascular beds. These effects complement GLP-1 agonists' anti-inflammatory and anti-atherosclerotic actions by addressing the metabolic component of cardiovascular risk at the cellular level.
SS-31 (Elamipretide) targets mitochondrial dysfunction, which is increasingly recognized as a contributor to heart failure, particularly HFpEF. By stabilizing the inner mitochondrial membrane and improving electron transport chain efficiency, SS-31 may enhance cardiac energy production in hearts that are metabolically stressed by obesity, diabetes, and aging. Clinical trials of SS-31 in heart failure are underway, with early results suggesting improvements in cardiac energetics and exercise capacity.
The peptide research hub provides comprehensive information on cardiovascular support peptides and their potential role as complements to GLP-1 therapy in a holistic cardiovascular risk management strategy.
GLP-1 Agonists and Stroke Prevention: Cerebrovascular Evidence and Neuroprotective Potential
While much of the cardiovascular discussion around GLP-1 agonists focuses on coronary artery disease and heart failure, the cerebrovascular evidence, specifically regarding stroke prevention and neuroprotection, deserves dedicated attention. Stroke remains the second leading cause of death worldwide and a major cause of long-term disability, and any intervention that reduces stroke risk has enormous public health significance.
Stroke Outcomes in GLP-1 Cardiovascular Trials
Stroke was included as a component of the major adverse cardiovascular events (MACE) endpoint in all GLP-1 agonist cardiovascular outcome trials. The stroke-specific results have been generally favorable but less statistically strong than the overall MACE results, primarily because stroke events were less frequent than myocardial infarction, limiting statistical power for stroke-specific analyses.
In the SUSTAIN-6 trial, semaglutide reduced non-fatal stroke by 39% compared to placebo (HR 0.61, 95% CI 0.38-0.99), a statistically significant finding that was one of the most striking results of the trial. In the SELECT trial, stroke was reduced by 7%, which was directionally favorable but not statistically significant. The LEADER trial showed a non-significant 14% reduction in non-fatal stroke with liraglutide.
Meta-analyses pooling stroke data across all GLP-1 agonist CVOTs have found a statistically significant overall reduction in stroke risk of approximately 15-17%, supporting a class effect of GLP-1 agonists on cerebrovascular outcomes. The mechanisms likely include reduced atherosclerosis in carotid and cerebral arteries (through the same anti-inflammatory and anti-atherogenic effects that protect coronary arteries), improved endothelial function in cerebral vessels, reduced blood pressure (a major modifiable stroke risk factor), and potentially direct neuroprotective effects of GLP-1 receptor activation in the brain.
Neuroprotective Mechanisms
GLP-1 receptors are widely expressed in the brain, including regions vulnerable to ischemic injury. Preclinical studies have consistently demonstrated that GLP-1 receptor activation reduces infarct size (the volume of brain tissue killed) in animal models of stroke, even when the GLP-1 agonist is administered after the stroke has occurred. The neuroprotective mechanisms include reduced excitotoxicity (GLP-1R activation attenuates glutamate-mediated neuronal death), enhanced anti-apoptotic signaling (through PI3K/Akt and MAPK pathways), reduced neuroinflammation (through microglial modulation), improved cerebral blood flow (through endothelial nitric oxide production), and promotion of neurogenesis and neural repair in the post-stroke period.
These preclinical findings have generated interest in GLP-1 agonists as acute neuroprotective agents for stroke treatment, not just for stroke prevention. Clinical trials testing exenatide in acute ischemic stroke are in early stages, though the translation from preclinical neuroprotection to clinical benefit has historically been challenging for other compounds. The ongoing research into GLP-1 agonists for both stroke prevention and acute neuroprotection represents a promising direction for cerebrovascular medicine. The GLP-1 research hub provides updates on cerebrovascular research and the broader cardiovascular evidence base for GLP-1 therapies.
Patient Communication About Cardiovascular Benefits
For many patients, the cardiovascular benefits of GLP-1 agonist therapy are invisible. Unlike weight loss (which patients can see and feel) or glycemic improvement (which appears on blood test results), cardiovascular protection operates silently in the background, preventing events that haven't happened yet. This invisibility creates a communication challenge for clinicians trying to motivate long-term treatment adherence for cardiovascular protection.
Effective patient communication about cardiovascular benefits focuses on concrete, relatable risk reduction. Rather than quoting hazard ratios and confidence intervals, clinicians can frame the benefit in personal terms: "Based on the SELECT trial, taking this medication for 3-4 years reduces your risk of having a heart attack or stroke by about 20%. For someone with your risk profile, that translates to preventing roughly 1 in 5 cardiac events that would otherwise occur." This personalized framing makes the statistical benefit tangible and motivating.
Patients who understand the cardiovascular benefit are more likely to continue therapy long-term, even if they reach their weight loss goals and are tempted to discontinue. The cardiovascular protection appears to require ongoing treatment (benefit curves in clinical trials plateau but don't continue to separate after treatment ends), which means that stopping GLP-1 therapy after reaching a target weight may sacrifice cardiovascular protection. This ongoing protection provides a compelling argument for indefinite therapy in patients with established cardiovascular disease, even when weight loss goals have been achieved.
GLP-1 Agonists and Peripheral Arterial Disease: The Overlooked Vascular Benefit
While much attention has focused on coronary and cerebrovascular outcomes, the effects of GLP-1 receptor agonists on peripheral arterial disease (PAD) represent a clinically meaningful but underexplored dimension of cardiovascular protection. PAD affects approximately 8-12% of the general adult population and up to 20-30% of patients with diabetes, making it one of the most common manifestations of systemic atherosclerosis. It is associated with reduced walking capacity, chronic leg pain, poor wound healing, and in severe cases, limb amputation. Patients with PAD also face markedly elevated risks of heart attack, stroke, and cardiovascular death, since the same atherosclerotic processes affecting the legs are typically present throughout the arterial tree.
Several lines of evidence suggest that GLP-1 receptor agonists could provide specific benefits for PAD patients. First, the anti-inflammatory and anti-atherosclerotic mechanisms described throughout this report apply equally to peripheral arteries. Macrophage modulation, plaque stabilization, and endothelial function improvement are systemic effects that benefit all vascular beds, not just coronary or cerebral arteries. Second, GLP-1 receptor agonists improve several PAD-specific risk factors, including hyperglycemia (which accelerates peripheral neuropathy and impairs wound healing), dyslipidemia (which drives plaque progression in peripheral vessels), and hypertension (which increases shear stress on already diseased arterial walls).
Preclinical research has provided more direct evidence. In mouse models of hindlimb ischemia (which mimic the reduced blood flow seen in PAD), treatment with GLP-1 receptor agonists increased angiogenesis and arteriogenesis, the formation of new blood vessels and the enlargement of existing collateral vessels that bypass arterial blockages. These effects appear to be mediated through GLP-1 receptor-dependent activation of endothelial nitric oxide synthase (eNOS), with downstream increases in vascular endothelial growth factor (VEGF) expression. If these findings translate to humans, GLP-1 therapy could improve blood flow to ischemic limbs through mechanisms beyond simple risk factor modification.
Clinical trial data, while limited, supports cautious optimism. Post-hoc analyses of the LEADER and SUSTAIN-6 trials showed trends toward reduced peripheral vascular events in patients randomized to liraglutide and semaglutide, though these analyses were not powered to reach statistical significance for PAD endpoints specifically. The SELECT trial included ankle-brachial index (ABI) measurements in a subset of patients, and preliminary data suggest improvements in ABI values with semaglutide treatment, indicating improved peripheral arterial perfusion. A dedicated PAD outcomes trial would be needed to confirm these signals, and several research groups have proposed such studies.
For patients with established PAD who are considering GLP-1 therapy for weight management or diabetes, the potential peripheral vascular benefits represent an additional consideration in the treatment decision. The weight loss associated with tirzepatide and semaglutide can improve walking capacity and reduce the mechanical stress on already compromised lower extremities, while the anti-inflammatory effects may help stabilize peripheral plaques and reduce the risk of acute limb ischemia. Clinicians managing PAD patients should consider these vascular benefits when evaluating the overall risk-benefit profile of GLP-1 receptor agonist therapy, particularly in patients who have both obesity and symptomatic peripheral vascular disease.
The wound healing dimension is also worth noting. PAD patients, especially those with diabetes, are at high risk for chronic non-healing wounds on the lower extremities. Improved peripheral perfusion, reduced systemic inflammation, and better glycemic control all contribute to wound healing capacity. Some vascular surgeons have begun anecdotally reporting improved surgical wound healing in PAD patients who are concurrently on GLP-1 therapy, though prospective data on this specific outcome is still lacking.
Frequently Asked Questions
Do GLP-1 receptor agonists actually reduce heart attack risk?
Yes, and the evidence is substantial. Across six major cardiovascular outcomes trials enrolling over 60,000 patients, GLP-1 receptor agonists reduced the composite of cardiovascular death, non-fatal heart attack, and non-fatal stroke by 14% on average. The SELECT trial specifically showed a 28% reduction in non-fatal myocardial infarction with semaglutide 2.4 mg in non-diabetic patients with obesity and established cardiovascular disease. The benefit appears to be driven by anti-atherosclerotic effects that stabilize plaques, anti-inflammatory actions that reduce plaque vulnerability, and direct protective effects on heart muscle during ischemic events. These reductions are on top of standard therapies including statins and antiplatelets.
What was the main finding of the SELECT trial?
SELECT was a landmark trial that enrolled 17,604 adults aged 45+ with BMI ≥27 and established atherosclerotic cardiovascular disease who did not have diabetes. Participants received semaglutide 2.4 mg weekly or placebo for a median of 39.8 months. The primary result was a 20% reduction in three-point MACE (cardiovascular death, non-fatal MI, non-fatal stroke) with semaglutide. All-cause mortality was reduced by 19%. This was the first trial to demonstrate GLP-1 RA cardiovascular benefit in a non-diabetic population, establishing that the heart benefits are not dependent on glucose lowering and opening the door to using semaglutide specifically as a cardiovascular risk reduction agent in patients with obesity.
Are the cardiovascular benefits of GLP-1 drugs just from weight loss?
No. Mediation analyses from SELECT estimate that only about 40% of the MACE reduction is explained by changes in body weight. The remaining 60% comes from weight-independent mechanisms including direct anti-inflammatory effects (reflected in roughly 38% CRP reduction), improved endothelial function and nitric oxide production, reduced oxidative stress, anti-thrombotic actions on platelets, and direct protective effects on heart muscle cells through GLP-1 receptors expressed in cardiac tissue. The early separation of cardiovascular event curves (within 3-6 months) before maximum weight loss is achieved, and the cardiovascular benefit in trials with relatively modest weight loss (like REWIND, with only 1.5 kg difference), both support the conclusion that GLP-1 RAs protect the heart through mechanisms beyond weight reduction.
Can GLP-1 drugs help with heart failure?
Yes, specifically for heart failure with preserved ejection fraction (HFpEF) in patients with obesity. The STEP-HFpEF trial showed that semaglutide 2.4 mg improved heart failure symptoms by 7.8 points more than placebo on the Kansas City Cardiomyopathy Questionnaire, a clinically meaningful difference. Exercise capacity also improved. The SUMMIT trial with tirzepatide went further, showing a 38% reduction in the composite of cardiovascular death and worsening heart failure events. The benefits are thought to come from reduced epicardial fat, decreased inflammation, improved diastolic function, and reduced fluid retention. For heart failure with reduced ejection fraction (HFrEF), the evidence is less clear and further studies are ongoing.
Do GLP-1 drugs protect against stroke?
GLP-1 receptor agonists have shown consistent signals for stroke reduction. The SUSTAIN-6 trial demonstrated a striking 39% reduction in non-fatal stroke with subcutaneous semaglutide. REWIND showed a 24% stroke reduction with dulaglutide. A meta-analysis across all GLP-1 RA CVOTs found a 17% overall reduction in non-fatal stroke. The mechanisms likely include blood pressure reduction (3-6 mmHg systolic), anti-atherosclerotic effects on carotid plaque, improved endothelial function in cerebral vasculature, and anti-thrombotic effects. These stroke-protective effects make GLP-1 RAs particularly valuable for patients with a history of cerebrovascular disease or significant carotid atherosclerosis.
How do the cardiovascular benefits compare between different GLP-1 drugs?
Semaglutide (subcutaneous) has the strongest cardiovascular evidence, with both SUSTAIN-6 (26% MACE reduction in T2D) and SELECT (20% MACE reduction in non-diabetic obesity) demonstrating superiority. Liraglutide showed a 13% MACE reduction in LEADER, with a significant mortality benefit. Dulaglutide achieved a 12% MACE reduction in REWIND, including primary prevention patients. Extended-release exenatide did not reach statistical significance in EXSCEL. Tirzepatide's cardiovascular outcomes trial (SURPASS-CVOT) is still underway, though SUMMIT demonstrated heart failure benefits. For patients where cardiovascular risk reduction is the primary goal, semaglutide is generally the first choice. For a detailed comparison, see our GLP-1 class overview.
Should non-diabetic patients take GLP-1 drugs for heart protection?
Based on SELECT, semaglutide 2.4 mg has demonstrated a 20% reduction in major cardiovascular events in non-diabetic patients with BMI ≥27 and established atherosclerotic cardiovascular disease. Clinical guidelines now support considering semaglutide for cardiovascular risk reduction in this population. However, this doesn't mean every overweight person needs a GLP-1 RA. The strongest indication is for patients with established ASCVD (prior heart attack, stroke, or peripheral artery disease) who also have overweight or obesity. For non-diabetic patients without established CVD, the evidence doesn't yet support GLP-1 RA use purely for cardiovascular prevention.
How quickly do the cardiovascular benefits appear?
Cardiovascular event curves begin to separate within 3-6 months of starting GLP-1 RA therapy, earlier than would be expected if the benefit were solely from weight loss. Anti-inflammatory effects (CRP reduction) begin within 2-4 weeks. Blood pressure improvements are apparent within the first month. Endothelial function (measured by flow-mediated dilation) improves within 4 weeks. However, the full magnitude of cardiovascular risk reduction builds over time, with event curves continuing to diverge throughout the treatment period. In SELECT, the benefit was evident at 6 months and progressively increased through 3+ years of follow-up, suggesting that longer treatment duration produces greater cumulative protection.
Is the increased heart rate with GLP-1 drugs harmful?
GLP-1 receptor agonists increase resting heart rate by an average of 2-4 beats per minute. This is a direct pharmacological effect caused by GLP-1 receptor activation in the sinoatrial node. Despite theoretical concerns about heart rate elevation, all clinical evidence shows net cardiovascular benefit. The MACE reductions in LEADER, SUSTAIN-6, REWIND, and SELECT all occurred despite this modest heart rate increase. Subgroup analyses controlling for heart rate change show that the cardiovascular benefit is maintained. The heart rate effect is generally not clinically significant and does not require dose adjustment or additional monitoring in most patients, though caution is warranted in patients with pre-existing tachyarrhythmias.
Can GLP-1 drugs reverse atherosclerosis?
There is growing evidence that GLP-1 RAs can stabilize and potentially partially reverse atherosclerotic plaques. Imaging studies using coronary CT angiography have shown that semaglutide reduces total coronary plaque volume by approximately 8% over 12 months, with a preferential reduction in non-calcified (lipid-rich) plaque. Animal studies show even more dramatic effects, with 25-30% reductions in aortic plaque area and improvements in plaque composition (thicker fibrous caps, smaller necrotic cores, reduced inflammation). However, "reversal" is a strong word. The current evidence suggests plaque stabilization and regression rather than complete resolution. The combination of plaque volume reduction, compositional improvement, and reduced plaque inflammation collectively makes existing plaques less likely to rupture and cause acute events.
Should I take a GLP-1 drug along with my statin?
GLP-1 RAs and statins work through entirely different mechanisms and their cardiovascular benefits are additive, not overlapping. Statins primarily lower LDL cholesterol and reduce atherosclerotic plaque burden, while GLP-1 RAs primarily target inflammation, endothelial function, weight, and blood pressure. In SELECT, 90% of participants were already on statins, and semaglutide still produced a 20% MACE reduction on top of statin therapy. Current guidelines recommend GLP-1 RAs as complementary to, not replacements for, statins and other proven cardiovascular therapies. If you're eligible for both, you should be taking both. They are addressing different aspects of cardiovascular risk.
What happens to cardiovascular protection if I stop taking a GLP-1 drug?
The cardiovascular benefits of GLP-1 RAs appear to require ongoing treatment. Data from the STEP extension studies show that weight regain, blood pressure increases, and inflammatory marker elevation occur within weeks to months of discontinuation. While no trial has directly measured cardiovascular events after GLP-1 RA withdrawal, the loss of anti-inflammatory and metabolic benefits strongly suggests that cardiovascular protection diminishes. For this reason, guidelines generally recommend long-term, potentially lifelong, GLP-1 RA therapy for cardiovascular indication, similar to how statins are prescribed for chronic use. If you need to discontinue for any reason, discuss alternative strategies with your provider to maintain cardiovascular risk management.
Are GLP-1 drugs safe for patients with existing heart disease?
Yes, GLP-1 receptor agonists have been extensively studied in patients with existing heart disease, and the evidence consistently shows net benefit. All six major CVOTs enrolled patients with established cardiovascular disease or high cardiovascular risk, and serious cardiovascular adverse events were lower in the GLP-1 RA groups compared to placebo. There is no signal for increased arrhythmia risk, worsened heart failure (except possibly in HFrEF, where evidence is limited), or other cardiac adverse effects. The main safety considerations are gastrointestinal side effects (nausea, vomiting, diarrhea), which can be managed with slow dose escalation. GLP-1 RAs should be used with caution in patients with severe gastroparesis and are contraindicated in patients with personal or family history of medullary thyroid carcinoma or MEN2 syndrome.
How do GLP-1 drugs compare to SGLT2 inhibitors for heart protection?
GLP-1 RAs and SGLT2 inhibitors are complementary cardiovascular therapies with somewhat different benefit profiles. GLP-1 RAs show stronger reductions in atherosclerotic events (MI and stroke), while SGLT2 inhibitors show stronger reductions in heart failure hospitalizations and renal progression. A meta-analysis found that GLP-1 RAs reduce MACE by 14% versus 11% for SGLT2 inhibitors, while SGLT2 inhibitors reduce heart failure hospitalization by 32% versus 11% for GLP-1 RAs. For patients with T2D and ASCVD, the combination of both drug classes is increasingly recommended, as they address different cardiovascular risk pathways. The choice of which to initiate first may depend on whether atherosclerotic events or heart failure is the dominant concern.
References
- Marso SP, Daniels GH, Tanaka K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311-322. DOI: 10.1056/NEJMoa1603827
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844. DOI: 10.1056/NEJMoa1607141
- Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet. 2019;394(10193):121-130. DOI: 10.1016/S0140-6736(19)31149-3
- Holman RR, Bethel MA, Mentz RJ, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2017;377(13):1228-1239. DOI: 10.1056/NEJMoa1612917
- Husain M, Birkenfeld AL, Donsmark M, et al. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2019;381(9):841-851. DOI: 10.1056/NEJMoa1901118
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221-2232. DOI: 10.1056/NEJMoa2307563
- Kosiborod MN, Abildstrom SZ, Borlaug BA, et al. Semaglutide in patients with heart failure with preserved ejection fraction and obesity. N Engl J Med. 2023;389(12):1069-1084. DOI: 10.1056/NEJMoa2306963
- Packer M, Zile MR, Kramer CM, et al. Tirzepatide for heart failure with preserved ejection fraction and obesity. N Engl J Med. 2025;392(5):427-437. DOI: 10.1056/NEJMoa2410753
- Sattar N, Lee MMY, Kristensen SL, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021;9(10):653-662. DOI: 10.1016/S2213-8587(21)00203-5
- Kristensen SL, Rorth R, Jhund PS, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019;7(10):776-785. DOI: 10.1016/S2213-8587(19)30249-9
- Nauck MA, Meier JJ, Cavender MA, et al. Cardiovascular actions and clinical outcomes with glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors. Circulation. 2017;136(9):849-870. DOI: 10.1161/CIRCULATIONAHA.117.028136
- Drucker DJ. The cardiovascular biology of glucagon-like peptide-1. Cell Metab. 2016;24(1):15-30. DOI: 10.1016/j.cmet.2016.06.009
- Ussher JR, Drucker DJ. Glucagon-like peptide 1 receptor agonists: cardiovascular benefits and mechanisms of action. Nat Rev Cardiol. 2023;20(7):463-474. DOI: 10.1038/s41569-023-00849-3
- Verma S, Poulter NR, Engstrom T, et al. Cardiovascular effects of GLP-1 receptor agonists: beyond glucose lowering. Eur Heart J. 2023;44(14):1216-1229. DOI: 10.1093/eurheartj/ehad123
- Kosiborod MN, Petrie MC, Borlaug BA, et al. Semaglutide in patients with obesity-related heart failure and type 2 diabetes. N Engl J Med. 2024;390(15):1394-1407. DOI: 10.1056/NEJMoa2313601
- Richards CD, Lincoff AM, Nicholls SJ, et al. Mediation analysis of semaglutide effects on cardiovascular outcomes in the SELECT trial. Lancet. 2024;403(10431):989-998. DOI: 10.1016/S0140-6736(24)00271-8
- Ban K, Noyan-Ashraf MH, Hoefer J, et al. Cardioprotective and vasodilatory actions of glucagon-like peptide 1 receptor are mediated through both glucagon-like peptide 1 receptor-dependent and -independent pathways. Circulation. 2008;117(18):2340-2350. DOI: 10.1161/CIRCULATIONAHA.107.739938
- Noyan-Ashraf MH, Momen MA, Ban K, et al. GLP-1R agonist liraglutide activates cytoprotective pathways and improves outcomes after experimental myocardial infarction in mice. Diabetes. 2009;58(4):975-983. DOI: 10.2337/db08-1193
- Bose AK, Mocanu MM, Carr RD, et al. Glucagon-like peptide 1 can directly protect the heart against ischemia/reperfusion injury. Diabetes. 2005;54(1):146-151. DOI: 10.2337/diabetes.54.1.146
- Lonborg J, Kelbaek H, Vejlstrup N, et al. Exenatide reduces reperfusion injury in patients with ST-segment elevation myocardial infarction. Eur Heart J. 2012;33(12):1491-1499. DOI: 10.1093/eurheartj/ehr309
- Arakawa M, Mita T, Azuma K, et al. Inhibition of monocyte adhesion to endothelial cells and attenuation of atherosclerotic lesion by a glucagon-like peptide-1 receptor agonist, exendin-4. Diabetes. 2010;59(4):1030-1037. DOI: 10.2337/db09-1694
- Rizzo M, Rizvi AA, Patti AM, et al. Liraglutide improves metabolic parameters and carotid intima-media thickness in diabetic patients with the metabolic syndrome: an 18-month prospective study. Cardiovasc Diabetol. 2016;15(1):162. DOI: 10.1186/s12933-016-0480-8
- Rakipovski G, Rolin B, Nohr J, et al. The GLP-1 analogs liraglutide and semaglutide reduce atherosclerosis in ApoE(-/-) and LDLr(-/-) mice by a mechanism that includes inflammatory pathways. JACC Basic Transl Sci. 2018;3(6):844-857. DOI: 10.1016/j.jacbts.2018.09.004
- Nauck MA, Quast DR, Wefers J, et al. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. 2021;46:101102. DOI: 10.1016/j.molmet.2020.101102
- Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. 2018;27(4):740-756. DOI: 10.1016/j.cmet.2018.03.001
- Ceriello A, Novials A, Ortega E, et al. Glucagon-like peptide 1 reduces endothelial dysfunction, inflammation, and oxidative stress induced by both hyperglycemia and hypoglycemia in type 1 diabetes. Diabetes Care. 2013;36(8):2346-2350. DOI: 10.2337/dc12-2469
- Hogan AE, Gaoatswe G, Lynch L, et al. Glucagon-like peptide 1 analogue therapy directly modulates innate immune-mediated inflammation in individuals with type 2 diabetes mellitus. Diabetologia. 2014;57(4):781-784. DOI: 10.1007/s00125-013-3145-0
- Tanaka A, Node K. Exploration of the clinical benefits of GLP-1 receptor agonists in diabetic patients with heart failure. Cardiovasc Diabetol. 2019;18(1):143. DOI: 10.1186/s12933-019-0949-z
- Marsico F, Paolillo S, Gargiulo P, et al. Effects of glucagon-like peptide-1 receptor agonists on major cardiovascular events in patients with type 2 diabetes mellitus with or without established cardiovascular disease: a meta-analysis of randomized controlled trials. Eur Heart J. 2020;41(35):3346-3358. DOI: 10.1093/eurheartj/ehaa082
- Green JB, Hernandez AF, D'Agostino RB, et al. Harmony Outcomes: a randomized, double-blind, placebo-controlled trial of the effect of albiglutide on major cardiovascular events in patients with type 2 diabetes mellitus. Lancet. 2018;392(10157):1519-1529. DOI: 10.1016/S0140-6736(18)32261-X
- Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377(12):1119-1131. DOI: 10.1056/NEJMoa1707914
- Helmstadter J, Frenis K, Filippou K, et al. Endothelial GLP-1 (glucagon-like peptide-1) receptor mediates cardiovascular protection by liraglutide in mice with experimental arterial hypertension. Arterioscler Thromb Vasc Biol. 2020;40(1):145-158. DOI: 10.1161/ATVBAHA.119.313474
- Ussher JR, Drucker DJ. Cardiovascular actions of incretin-based therapies. Circ Res. 2014;114(11):1788-1803. DOI: 10.1161/CIRCRESAHA.114.301958
- Lambadiari V, Pavlidis G, Kousathana F, et al. Effects of 6-month treatment with the glucagon like peptide-1 analogue liraglutide on arterial stiffness, left ventricular myocardial deformation and oxidative stress in subjects with newly diagnosed type 2 diabetes. Cardiovasc Diabetol. 2018;17(1):8. DOI: 10.1186/s12933-017-0646-z
- Bethel MA, Patel RA, Merrill P, et al. Cardiovascular outcomes with glucagon-like peptide-1 receptor agonists in patients with type 2 diabetes: a meta-analysis. Lancet Diabetes Endocrinol. 2018;6(2):105-113. DOI: 10.1016/S2213-8587(17)30412-6
- Iacobellis G, Villasante Fricke AC. Effects of semaglutide versus dulaglutide on epicardial fat thickness in subjects with type 2 diabetes and obesity. J Endocr Soc. 2020;4(4):bvz042. DOI: 10.1210/jendso/bvz042
- Almutairi M, Gopal K, Engelbrecht E, et al. GLP-1 receptor agonism recovers impaired cardiac glucose metabolism in a murine model of obesity. Diabetes. 2023;72(Suppl 1):83-OR. DOI: 10.2337/db23-83-OR
- American Diabetes Association Professional Practice Committee. Cardiovascular disease and risk management: Standards of Care in Diabetes - 2025. Diabetes Care. 2025;48(Suppl 1):S207-S238. DOI: 10.2337/dc25-S010
- Marx N, Federici M, Schutt K, et al. 2023 ESC guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J. 2023;44(39):4043-4140. DOI: 10.1093/eurheartj/ehad192
- Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the management of patients with chronic coronary disease. Circulation. 2023;148(24):e364-e458. DOI: 10.1161/CIR.0000000000001168
- Verma S, Bain SC, Monk Fries T, et al. Duration of diabetes and cardiorenal efficacy of liraglutide and semaglutide: a post hoc analysis of the LEADER and SUSTAIN 6 clinical trials. Diabetes Obes Metab. 2019;21(7):1745-1751. DOI: 10.1111/dom.13722
- Frias JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med. 2021;385(6):503-515. DOI: 10.1056/NEJMoa2107519
- Margulies KB, Hernandez AF, Redfield MM, et al. Effects of liraglutide on clinical stability among patients with advanced heart failure and reduced ejection fraction: a randomized clinical trial. JAMA. 2016;316(5):500-508. DOI: 10.1001/jama.2016.10260
- Patel KV, Segar MW, Lavie CJ, et al. Diabetes status modifies the association between different measures of obesity and heart failure risk among older adults: a pooled analysis of community-based NHLBI cohorts. Circulation. 2022;145(4):268-278. DOI: 10.1161/CIRCULATIONAHA.121.055830
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183
- Look AHEAD Research Group. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013;369(2):145-154. DOI: 10.1056/NEJMoa1212914
- Sjostrom L, Peltonen M, Jacobson P, et al. Association of bariatric surgery with long-term remission of type 2 diabetes and with microvascular and macrovascular complications. JAMA. 2014;311(22):2297-2304. DOI: 10.1001/jama.2014.5988
- Kosiborod MN, Verma S, Borlaug BA, et al. Effects of semaglutide on symptoms, function, and quality of life in patients with heart failure with preserved ejection fraction and obesity: a prespecified analysis of the STEP-HFpEF trial. Circulation. 2024;149(3):204-216. DOI: 10.1161/CIRCULATIONAHA.123.067505
- Husain M, Bain SC, Jeppesen OK, et al. Semaglutide (SUSTAIN and PIONEER) reduces cardiovascular events in type 2 diabetes across varying cardiovascular risk. Diabetes Obes Metab. 2020;22(3):442-451. DOI: 10.1111/dom.13901
- Newsome PN, Buchholtz K, Cusi K, et al. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. N Engl J Med. 2021;384(12):1113-1124. DOI: 10.1056/NEJMoa2028395
- Gerstein HC, Sattar N, Engstrom T, et al. Growth differentiation factor 15 and cardiovascular outcomes in patients with type 2 diabetes: results from the REWIND trial. Eur Heart J. 2024;45(1):78-88. DOI: 10.1093/eurheartj/ehad578
- Pratley RE, Aroda VR, Lingvay I, et al. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol. 2018;6(4):275-286. DOI: 10.1016/S2213-8587(18)30024-X
- Baggio LL, Yusta B, Mulvihill EE, et al. GLP-1 receptor expression within the human heart. Endocrinology. 2018;159(4):1570-1584. DOI: 10.1210/en.2018-00004
- Kim M, Platt MJ, Shiber T, et al. GLP-1 receptor activation and Epac2 link atrial natriuretic peptide secretion to control of blood pressure. Nat Med. 2013;19(5):567-575. DOI: 10.1038/nm.3128
- Wroge CM, Segar MW, Engstrom T, et al. GLP-1 receptor agonists and cardiorenal outcomes by baseline kidney function: a meta-analysis of cardiovascular outcomes trials. Kidney Int. 2024;105(4):835-845. DOI: 10.1016/j.kint.2024.01.013
- Giugliano D, Scappaticcio L, Longo M, et al. GLP-1 receptor agonists and cardiorenal outcomes in type 2 diabetes: an updated meta-analysis of eight CVOTs. Cardiovasc Diabetol. 2021;20(1):189. DOI: 10.1186/s12933-021-01366-8
- Moura FA, Berg DD, Engstrom T, et al. Cardiovascular and metabolic effects of semaglutide in patients with overweight or obesity and cardiovascular disease: the SELECT biomarker substudy. Circulation. 2024;149(12):923-933. DOI: 10.1161/CIRCULATIONAHA.123.067928
- Leiter LA, Bain SC, Hramiak I, et al. Cardiovascular risk reduction with once-weekly semaglutide in subjects with type 2 diabetes: a post hoc analysis of gender, age, and baseline CV risk profile in the SUSTAIN 6 trial. Cardiovasc Diabetol. 2019;18(1):73. DOI: 10.1186/s12933-019-0871-8
- Shah M, Vella A. Effects of GLP-1 on appetite and weight. Rev Endocr Metab Disord. 2014;15(3):181-187. DOI: 10.1007/s11154-014-9289-5
- Nauck MA, D'Alessio DA. Tirzepatide, a dual GIP/GLP-1 receptor co-agonist for the treatment of type 2 diabetes with unmatched effectiveness regarding reduction of HbA1c and body weight. Cardiovasc Diabetol. 2022;21(1):169. DOI: 10.1186/s12933-022-01604-7
- Neves JS, Packer M, Ferreira JP. GLP-1 receptor agonists in heart failure: current evidence and future directions. Cardiovasc Drugs Ther. 2024;38(1):109-120. DOI: 10.1007/s10557-023-07529-4
- Kosiborod MN, Deanfield JE, Engstrom T, et al. Semaglutide and cardiovascular outcomes by baseline blood pressure in the SELECT trial. JAMA Cardiol. 2024;9(8):719-728. DOI: 10.1001/jamacardio.2024.1579