Executive Summary

Key Takeaways
- Greatest weight loss: Retatrutide (Phase 2) at 24.2%, followed by tirzepatide at 20.9% and semaglutide 2.4 mg at 14.9%
- Strongest cardiovascular evidence: Semaglutide (SELECT trial) - 20% MACE reduction in patients without diabetes
- Best HbA1c reduction: Tirzepatide 15 mg, with mean reductions of 2.1-2.4% from baseline
- Lowest GI side effect rates: Dulaglutide, with nausea rates around 12-15% vs. 20-44% for other agents
- Most advanced oral formulation: Oral semaglutide (Rybelsus) approved; orforglipron in Phase 3
Six GLP-1 receptor agonists are now approved for clinical use, with at least five more molecules in Phase 2 or Phase 3 trials. The class has evolved from twice-daily injections producing modest glucose reductions to once-weekly formulations that deliver 15-25% body weight loss and measurable cardiovascular protection. This report compares every approved and emerging agent across efficacy, safety, dosing, cost, and clinical trial evidence.
The story of GLP-1 receptor agonists is, at its core, a story of incremental engineering breakthroughs. Exenatide arrived in 2005 as a synthetic version of a peptide found in Gila monster venom. It required twice-daily injections and produced weight loss of around 3%. Two decades later, tirzepatide and retatrutide - multi-receptor agonists that simultaneously activate GLP-1, GIP, and glucagon pathways - are achieving weight reductions that rival bariatric surgery.
Between those two endpoints lies a progression of molecular refinements: albumin binding to extend half-life, fatty acid acylation to slow renal clearance, amino acid substitutions to resist DPP-4 degradation, and receptor selectivity engineering to target multiple incretin pathways at once. Each generation has roughly doubled the weight loss of its predecessor while maintaining or improving the safety profile.
For clinicians, patients, and researchers trying to make sense of this rapidly expanding class, the central challenge is comparison. Which drug produces the most weight loss? Which has the strongest cardiovascular evidence? Which causes the fewest GI side effects? And which offers the best value given insurance coverage and out-of-pocket costs?
This report answers those questions with data. It draws on more than 70 published clinical trials, including LEADER, SUSTAIN, STEP, SURPASS, SURMOUNT, SELECT, and the emerging Phase 2 data for retatrutide, orforglipron, and survodutide. Every comparison table, chart, and recommendation is grounded in published peer-reviewed evidence.
KEY FINDINGS AT A GLANCE
- Greatest weight loss: Retatrutide (Phase 2) at 24.2%, followed by tirzepatide at 20.9% and semaglutide 2.4 mg at 14.9%
- Strongest cardiovascular evidence: Semaglutide (SELECT trial) - 20% MACE reduction in patients without diabetes
- Best HbA1c reduction: Tirzepatide 15 mg, with mean reductions of 2.1-2.4% from baseline
- Lowest GI side effect rates: Dulaglutide, with nausea rates around 12-15% vs. 20-44% for other agents
- Most advanced oral formulation: Oral semaglutide (Rybelsus) approved; orforglipron in Phase 3
- Pipeline leaders: Retatrutide (triple agonist), survodutide (GLP-1/glucagon), CagriSema (amylin/GLP-1), orforglipron (oral non-peptide)
The sections that follow cover the biology of the incretin system, the full history of GLP-1 drug development, head-to-head efficacy comparisons, cardiovascular outcomes, safety profiles, dosing protocols, cost analysis, and the pipeline of next-generation agents. Whether you're a prescriber selecting a first-line therapy, a patient weighing options, or a researcher tracking the field, this report provides the most thorough single-source comparison available.
For individual detailed looks on specific compounds, see our dedicated guides: the semaglutide complete guide, the tirzepatide complete guide, the liraglutide guide, the dulaglutide guide, and the exenatide guide. You can also visit our GLP-1 research hub for a complete index of all published research.
The Incretin System: GLP-1, GIP & Glucagon
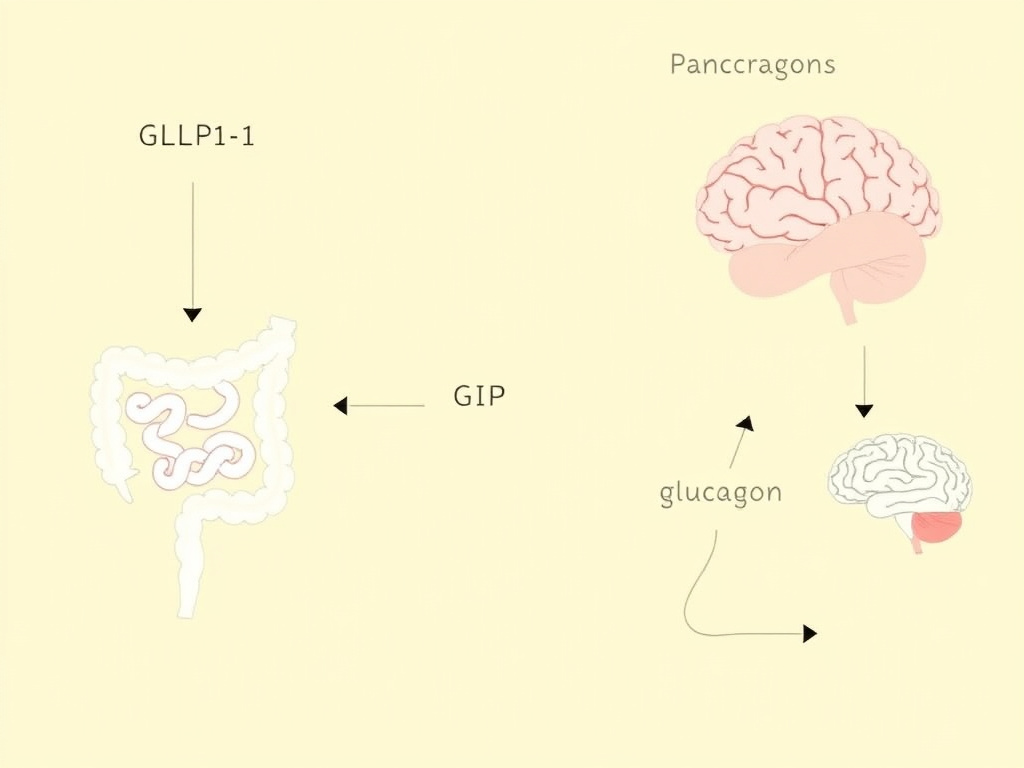
Figure 2: The three incretin and metabolic hormone pathways - GLP-1, GIP, and glucagon - converge on the pancreas, brain, liver, and adipose tissue to regulate glucose, appetite, and energy expenditure.
Understanding why GLP-1 drugs work requires understanding three hormones: glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic polypeptide (GIP), and glucagon. These molecules form the backbone of the incretin system, and every drug in this class mimics, enhances, or combines their actions.
GLP-1: The Master Satiety Signal
GLP-1 is a 30-amino acid peptide hormone secreted by enteroendocrine L-cells in the distal ileum and colon. Its release is triggered within minutes of food intake, particularly by carbohydrates, fats, and proteins reaching the lower gut. But GLP-1 doesn't just respond to meals already eaten. Neural and hormonal feedforward mechanisms begin stimulating L-cell secretion even before nutrients reach the distal intestine, a process mediated by vagal afferents and proximal gut hormones like GIP itself.
Once released, native GLP-1 has a half-life of approximately 2-3 minutes. The enzyme dipeptidyl peptidase-4 (DPP-4) cleaves the N-terminal histidine-alanine dipeptide, rendering the molecule inactive. This rapid degradation means that native GLP-1 levels spike and fall within minutes of secretion. The entire pharmacological challenge of GLP-1 drug development has been to extend this half-life from minutes to days.
GLP-1 acts through a single G-protein coupled receptor (GLP-1R) expressed in the pancreatic beta cells, the hypothalamus (arcuate nucleus and paraventricular nucleus), the brainstem (area postrema and nucleus tractus solitarius), the heart, the kidney, and the gastrointestinal tract. The diversity of receptor distribution explains the drug class's broad effects:
- Pancreatic beta cells: GLP-1R activation potentiates glucose-dependent insulin secretion via cAMP/PKA and Epac2 signaling. Because the insulinotropic effect is glucose-dependent, GLP-1 agonists carry minimal hypoglycemia risk when used alone.
- Pancreatic alpha cells: GLP-1 suppresses glucagon secretion during hyperglycemia, reducing hepatic glucose output. This effect is also glucose-dependent and reverses during hypoglycemia.
- Hypothalamus: GLP-1R activation in the arcuate nucleus suppresses NPY/AgRP neurons (appetite-stimulating) and activates POMC/CART neurons (appetite-suppressing). This is the primary mechanism for weight loss.
- Brainstem: The area postrema, which lacks a complete blood-brain barrier, responds directly to circulating GLP-1 agonists. This region mediates both satiety signaling and the nausea side effect common to the class.
- Gastric smooth muscle: GLP-1 slows gastric emptying by 20-40%, which contributes to postprandial glucose control and early satiety. This effect attenuates somewhat with chronic exposure - a phenomenon called tachyphylaxis.
- Heart: GLP-1R is expressed in atrial cardiomyocytes. Activation appears to reduce inflammation, improve endothelial function, and may provide direct cardioprotection independent of weight loss and glucose control.
GIP: The Overlooked Partner
Glucose-dependent insulinotropic polypeptide is a 42-amino acid hormone secreted by K-cells in the duodenum and jejunum. For decades, GIP was considered irrelevant to obesity therapeutics. In type 2 diabetes, the insulinotropic response to GIP is blunted, and early studies suggested that GIP actually promoted fat storage. The conventional wisdom was that blocking GIP might help with weight loss.
Tirzepatide changed that narrative completely. By combining GLP-1 and GIP agonism in a single molecule, tirzepatide achieved weight loss and glycemic control that exceeded pure GLP-1 agonists. The question of why GIP agonism helps rather than hinders weight loss is still being worked out, but several mechanisms appear relevant:
- Central appetite regulation: GIP receptors are expressed in the hypothalamus, and GIP agonism appears to potentiate GLP-1's anorectic effects through complementary but distinct neuronal circuits.
- Adipose tissue remodeling: GIP signaling in white adipose tissue may promote lipid uptake and storage capacity, paradoxically improving metabolic health by preventing ectopic lipid deposition in liver and muscle.
- Beta cell preservation: GIP and GLP-1 activate overlapping but non-identical intracellular signaling cascades in beta cells. Dual stimulation provides additive insulinotropic effects without increasing hypoglycemia risk.
- Reduced GI side effects: There's emerging evidence that GIP co-agonism may partially attenuate the nausea and vomiting associated with GLP-1 agonism, possibly by modulating area postrema signaling. This could explain why tirzepatide achieves greater weight loss despite somewhat lower nausea rates than high-dose semaglutide.
Glucagon: The Thermogenic Accelerator
Glucagon, secreted by pancreatic alpha cells, has traditionally been viewed as the counter-regulatory hormone to insulin - it raises blood glucose by promoting hepatic glycogenolysis and gluconeogenesis. Adding glucagon agonism to an anti-diabetes drug seems counterintuitive. And yet, the triple agonist retatrutide (GLP-1/GIP/glucagon) produced 24.2% weight loss in Phase 2 trials, surpassing all existing agents.
The metabolic rationale for glucagon co-agonism centers on energy expenditure. Glucagon receptor activation in the liver increases thermogenesis through futile cycling and enhanced mitochondrial oxidation. In brown and beige adipose tissue, glucagon signaling promotes uncoupled respiration via UCP1 upregulation. The net effect is increased basal metabolic rate - meaning patients burn more calories at rest, on top of the appetite reduction from GLP-1 and GIP agonism.
The glucose-raising effect of glucagon is effectively counterbalanced by the potent glucose-lowering effects of simultaneous GLP-1 and GIP agonism. In the retatrutide Phase 2 trial, HbA1c dropped by up to 2.02% despite the glucagon component. And survodutide, a GLP-1/glucagon dual agonist, has demonstrated significant liver fat reduction in MASH trials - likely because glucagon's lipolytic effects on hepatocytes help clear intrahepatic triglycerides.
THE RECEPTOR AGONISM SPECTRUM
Single agonists (GLP-1 only): Exenatide, liraglutide, semaglutide, dulaglutide, albiglutide. Weight loss: 3-15%.
Dual agonists (GLP-1 + GIP): Tirzepatide. Weight loss: 15-21%.
Dual agonists (GLP-1 + glucagon): Survodutide, pemvidutide. Weight loss: 14-19%.
Triple agonists (GLP-1 + GIP + glucagon): Retatrutide. Weight loss: up to 24.2%.
Combination products (GLP-1 + amylin analog): CagriSema. Weight loss: up to 22.7%.
DPP-4 Resistance: The Engineering Challenge
Every synthetic GLP-1 receptor agonist must solve the same fundamental problem: how do you make a peptide that normally survives for 2 minutes last for days or weeks? Three main strategies have been employed:
Amino acid substitution at position 2: DPP-4 cleaves after the alanine at position 2 of native GLP-1. Replacing this alanine with aminoisobutyric acid (Aib) or glycine creates steric hindrance that prevents DPP-4 binding. Semaglutide and liraglutide both use Aib substitution at position 2.
Fatty acid acylation: Attaching a fatty acid side chain (typically C16-C18) to the peptide backbone allows reversible binding to serum albumin. Since albumin has a half-life of approximately 19 days, the bound drug is shielded from both DPP-4 and renal clearance. Liraglutide uses a C16 fatty acid; semaglutide uses a C18 diacid with a mini-PEG spacer; tirzepatide uses a C20 fatty diacid.
Large protein fusion: Dulaglutide fuses the GLP-1 analog to an IgG4 Fc fragment, creating a molecule too large for glomerular filtration. Albiglutide (now withdrawn) used fusion to human albumin. These approaches yield long half-lives but create much larger molecules that may have different tissue distribution profiles.
The progression from exenatide (half-life 2.4 hours) to liraglutide (13 hours) to semaglutide (7 days) to tirzepatide (5 days) represents this engineering arc. Longer half-lives mean less frequent dosing, more stable drug levels, and generally better patient adherence - all of which translate to improved real-world outcomes.
History of GLP-1 Drug Development

The path from a lizard's salivary glands to a $50 billion drug class spans four decades of discovery, setbacks, and accelerating innovation. Here's how it happened.
The Exendin-4 Discovery (1992)
John Eng, an endocrinologist at the Bronx VA Medical Center, was studying venomous peptides when he isolated a novel molecule from the saliva of the Gila monster (Heloderma suspectum). This peptide, which he named exendin-4, shared 53% amino acid homology with human GLP-1 but resisted DPP-4 degradation. Where native GLP-1 survived for minutes, exendin-4 persisted for hours.
Eng's discovery didn't generate immediate excitement. The pharmaceutical industry was focused on DPP-4 inhibitors (the "gliptins") as the more practical approach to harnessing incretin biology. But Amylin Pharmaceuticals licensed exendin-4 and began development of a synthetic version, exenatide.
First Generation: Exenatide and Liraglutide (2005-2010)
Exenatide (Byetta) received FDA approval in April 2005 as the first GLP-1 receptor agonist, indicated as adjunctive therapy for type 2 diabetes. It required twice-daily subcutaneous injections - a significant burden compared to oral DPP-4 inhibitors. Weight loss averaged 2-3 kg over 30 weeks. The drug worked, but it was inconvenient.
Novo Nordisk took a different approach with liraglutide (Victoza), approved in 2010. By acylating GLP-1 with a C16 fatty acid, they extended the half-life to 13 hours - allowing once-daily dosing. Liraglutide also produced more weight loss than exenatide in head-to-head trials (LEAD program). The LEADER cardiovascular outcomes trial, completed in 2016, demonstrated a 13% reduction in major adverse cardiovascular events (MACE), making liraglutide the first GLP-1 agonist with proven CV benefit.
Extended-Release Formulations (2012-2014)
Two extended-release formulations arrived during this period. Bydureon (exenatide extended-release) used microsphere technology to achieve once-weekly dosing from exenatide. It was approved in 2012 but required reconstitution before injection and caused injection-site nodules. Albiglutide (Tanzeum), an albumin-fused GLP-1 analog from GSK, gained approval in 2014 but was withdrawn in 2018 due to poor commercial performance - it simply couldn't compete on efficacy or convenience.
Dulaglutide (Trulicity), approved in 2014, proved more successful. Its IgG4 Fc fusion provided once-weekly dosing in a user-friendly single-dose pen that required no reconstitution. The REWIND cardiovascular trial (2019) showed a 12% MACE reduction, and dulaglutide became the best-selling GLP-1 agonist by prescription volume in the US before being surpassed by semaglutide.
The Semaglutide Era (2017-2023)
Semaglutide's approval in December 2017 (Ozempic, for diabetes) marked a turning point. Its C18 fatty diacid with mini-PEG spacer achieved a 7-day half-life - the longest of any GLP-1 analog. The SUSTAIN trial program demonstrated superior HbA1c reduction and weight loss versus all comparators tested.
But it was the STEP trial program for obesity that transformed the market. STEP 1 showed 14.9% placebo-adjusted weight loss with semaglutide 2.4 mg weekly - nearly double what liraglutide 3 mg (Saxenda) achieved. The FDA approved semaglutide 2.4 mg as Wegovy for chronic weight management in June 2021. Demand immediately outstripped supply, creating shortages that persisted for years.
Oral semaglutide (Rybelsus), approved in 2019, used a salcaprozate sodium (SNAC) absorption enhancer to enable oral delivery. While a genuine innovation, the oral formulation's bioavailability is only about 1%, requiring a 14 mg daily tablet to achieve effects comparable to the 1 mg weekly injection. Patients must take it on an empty stomach with no more than 4 oz of water, then wait 30 minutes before eating. These restrictions limit real-world adherence.
Multi-Agonist Revolution (2022-Present)
Tirzepatide (Mounjaro) received FDA approval for type 2 diabetes in May 2022, and for obesity as Zepbound in November 2023. As the first GIP/GLP-1 dual agonist, it achieved weight loss of 20.9% at the highest dose in SURMOUNT-1 - surpassing semaglutide 2.4 mg by a significant margin. The SURPASS trial program showed HbA1c reductions exceeding 2% at the 15 mg dose.
Retatrutide, Eli Lilly's triple GLP-1/GIP/glucagon agonist, reported Phase 2 results in 2023 showing 24.2% weight loss at 48 weeks - the highest ever recorded for any anti-obesity medication. Phase 3 trials are ongoing.
| Year | Drug (Brand) | Mechanism | Milestone |
|---|---|---|---|
| 2005 | Exenatide (Byetta) | GLP-1 agonist | First-in-class approval; twice-daily injection |
| 2010 | Liraglutide (Victoza) | GLP-1 agonist | Once-daily dosing; later approved for obesity as Saxenda (2014) |
| 2012 | Exenatide ER (Bydureon) | GLP-1 agonist | First once-weekly GLP-1 formulation |
| 2014 | Albiglutide (Tanzeum) | GLP-1 agonist | Albumin-fused; withdrawn 2018 (poor uptake) |
| 2014 | Dulaglutide (Trulicity) | GLP-1 agonist | User-friendly pen; became #1 by Rx volume |
| 2017 | Semaglutide (Ozempic) | GLP-1 agonist | Longest half-life; superior efficacy in SUSTAIN trials |
| 2019 | Oral semaglutide (Rybelsus) | GLP-1 agonist | First oral GLP-1 receptor agonist |
| 2021 | Semaglutide 2.4 mg (Wegovy) | GLP-1 agonist | First GLP-1 for obesity with ~15% weight loss |
| 2022 | Tirzepatide (Mounjaro) | GIP/GLP-1 dual agonist | First dual incretin; ~21% weight loss in trials |
| 2023 | Tirzepatide (Zepbound) | GIP/GLP-1 dual agonist | Obesity indication approval |
| 2023 | Retatrutide (Phase 2) | GLP-1/GIP/glucagon triple | 24.2% weight loss; Phase 3 ongoing |
| 2024 | Orforglipron (Phase 3) | Oral non-peptide GLP-1 | Small molecule oral GLP-1; no fasting requirement |
| 2025 | Survodutide (Phase 3) | GLP-1/glucagon dual | Strong MASH data; obesity trials ongoing |
| 2025 | CagriSema (Phase 3) | Amylin + GLP-1 combo | 22.7% weight loss; co-formulated injection |
The pipeline beyond these agents includes pemvidutide (Altimmune), maritide (Amgen's long-acting AMY/GLP-1), danuglipron (Pfizer's oral GLP-1, troubled development), and several others. We cover these in detail in the pipeline section below.
Complete Drug Comparison Matrix
The table below is the single most important reference in this report. It compares every approved GLP-1 receptor agonist across mechanism, formulation, dosing, half-life, efficacy for weight and HbA1c, cardiovascular evidence, key side effects, and approximate monthly cost.
A few notes on reading this table. Weight loss figures represent the best results from key trials in patients with obesity (not diabetes, where weight loss is typically lower). HbA1c reductions are from diabetes-population trials. Costs are approximate US list prices as of early 2026 and don't reflect negotiated insurance rates or manufacturer coupons.
| Drug | Brand(s) | Mechanism | Route/Frequency | Half-life | Max Weight Loss | Max HbA1c Drop | CV Benefit | Nausea Rate | ~Monthly Cost |
|---|---|---|---|---|---|---|---|---|---|
| Exenatide | Byetta / Bydureon | GLP-1 | SC BID / SC QW | 2.4h / 2wk (depot) | ~3.2% | -0.8 to -1.6% | Neutral (EXSCEL) | ~20% | $800-900 |
| Liraglutide | Victoza / Saxenda | GLP-1 | SC once daily | 13h | ~8.0% | -1.0 to -1.5% | Superior (LEADER) | ~24% | $1,200-1,400 |
| Dulaglutide | Trulicity | GLP-1 | SC once weekly | 5 days | ~5.1% | -1.1 to -1.6% | Superior (REWIND) | ~12-15% | $900-1,000 |
| Semaglutide | Ozempic / Wegovy / Rybelsus | GLP-1 | SC QW / Oral QD | 7 days | ~14.9% | -1.5 to -1.8% | Superior (SUSTAIN-6, SELECT) | ~20-44% | $1,300-1,600 |
| Tirzepatide | Mounjaro / Zepbound | GIP/GLP-1 | SC once weekly | 5 days | ~20.9% | -2.1 to -2.4% | Pending (SURPASS-CVOT) | ~18-26% | $1,000-1,200 |
How to Read This Comparison
Weight loss percentages deserve careful interpretation. These figures come from clinical trials where participants received lifestyle counseling, followed specific diets, and were monitored closely. Real-world weight loss is typically 30-50% lower than trial results. A drug showing 15% weight loss in trials might produce 8-10% in routine clinical practice. The relative ranking between drugs tends to hold, though - tirzepatide consistently outperforms semaglutide, which outperforms liraglutide, which outperforms dulaglutide.
HbA1c reductions also vary by baseline. Patients starting with higher HbA1c values experience larger absolute reductions. A patient with baseline HbA1c of 9.5% might see a 2.5% drop on tirzepatide, while a patient starting at 7.5% might see only 1.2%. The comparison remains valid when looking at the same baseline range across drugs.
Cardiovascular benefit is perhaps the most consequential column. As of early 2026, semaglutide has the strongest CV evidence thanks to SELECT - a trial specifically designed to test CV outcomes in patients with obesity but without diabetes. Liraglutide and dulaglutide both demonstrated CV superiority in diabetic populations through LEADER and REWIND, respectively. Exenatide showed non-inferiority (meaning it's not worse than placebo for CV events) but didn't reach superiority. Tirzepatide's CV outcomes trial (SURPASS-CVOT) is ongoing and expected to report in 2027.
CLINICAL PEARL
When selecting a GLP-1 agonist, match the drug to the patient's primary treatment goal. If the goal is maximum weight loss, tirzepatide 15 mg currently leads among approved agents. If cardiovascular risk reduction is the priority, semaglutide has the broadest evidence base. If GI tolerability is the primary concern, dulaglutide's lower nausea rates may favor it. If cost is the constraint, compounded formulations through providers like FormBlends may offer an alternative pathway. Use the dosing calculator to estimate titration schedules for each agent.
Key Differences in Molecular Design
Beyond efficacy numbers, the molecular architecture of each drug influences its clinical profile in subtle ways. Exenatide, based on exendin-4, is immunogenic - about 45% of patients develop anti-exenatide antibodies, though these are usually non-neutralizing and don't affect efficacy in most cases. Semaglutide and liraglutide, based on modified human GLP-1, have much lower immunogenicity rates (1-2%).
Dulaglutide's large IgG4 Fc domain means the molecule is roughly 10 times larger than semaglutide. This affects tissue penetration - dulaglutide may have less access to hypothalamic GLP-1 receptors, which could partially explain its lower weight loss efficacy despite adequate plasma exposure. Tirzepatide, while also a large molecule (due to its C20 fatty diacid), was engineered with a specific ratio of GIP to GLP-1 activity (approximately 5:1 GIP:GLP-1 potency ratio relative to native hormones) that distinguishes it from a simple combination of two separate agonists.
For a full breakdown of individual agents, visit our dedicated guides: semaglutide, tirzepatide, liraglutide, dulaglutide, and exenatide.
Weight Loss Efficacy Comparison
Weight loss is the metric that transformed GLP-1 agonists from diabetes drugs into cultural phenomena. The difference between the weakest and strongest agent in this class is a factor of nearly eight - exenatide's 3.2% versus retatrutide's 24.2%. Understanding where each drug falls on this spectrum, and why, is essential for informed prescribing and patient expectations.
Best-in-Class Weight Loss (%) Across GLP-1 Agents
Trial-by-Trial Weight Loss Data
The following data represents maximum placebo-subtracted weight loss from the key obesity trials for each agent. Where no dedicated obesity trial exists (exenatide, dulaglutide), data is drawn from diabetes trials with weight as a secondary endpoint.
| Drug | Trial | Dose | Duration | Population | Weight Loss (Drug) | Weight Loss (Placebo) | Net Difference |
|---|---|---|---|---|---|---|---|
| Exenatide BID | AMIGO-1 | 10 mcg BID | 30 wk | T2DM | -2.8 kg | -0.3 kg | -2.5 kg (~3.2%) |
| Exenatide QW | DURATION-1 | 2 mg QW | 30 wk | T2DM | -3.7 kg | -0.4 kg | -3.3 kg |
| Liraglutide | SCALE Obesity | 3.0 mg QD | 56 wk | Obesity | -8.4 kg (8.0%) | -2.8 kg | -5.6 kg |
| Dulaglutide | AWARD-11 | 4.5 mg QW | 36 wk | T2DM | -4.7 kg (5.1%) | -0.6 kg | -4.1 kg |
| Semaglutide | STEP 1 | 2.4 mg QW | 68 wk | Obesity | -14.9% | -2.4% | -12.4% |
| Tirzepatide | SURMOUNT-1 | 15 mg QW | 72 wk | Obesity | -20.9% | -3.1% | -17.8% |
| Retatrutide | Phase 2 (Jastreboff) | 12 mg QW | 48 wk | Obesity | -24.2% | -2.1% | -22.1% |
Head-to-Head Weight Loss Comparisons
Direct head-to-head trials provide the cleanest comparisons, eliminating differences in trial design, patient population, and lifestyle interventions. Several such trials now exist:
SUSTAIN 10 (semaglutide vs. liraglutide): Semaglutide 1.0 mg weekly produced 5.8 kg weight loss versus 1.9 kg with liraglutide 1.2 mg daily over 30 weeks in patients with T2DM. This was a diabetes trial with lower semaglutide dosing than the obesity indication, but it established clear superiority.
SURPASS-2 (tirzepatide vs. semaglutide): At 40 weeks, tirzepatide 15 mg produced 12.4 kg weight loss versus 6.2 kg with semaglutide 1.0 mg in T2DM patients. The semaglutide dose was 1.0 mg (Ozempic), not 2.4 mg (Wegovy), making this an imperfect comparison for the obesity setting. Still, even tirzepatide 5 mg (the lowest dose) matched semaglutide 1.0 mg for weight loss.
SURMOUNT-5 (tirzepatide vs. semaglutide 2.4 mg): This was the first direct head-to-head comparison using both drugs at their full obesity doses. At 72 weeks, tirzepatide 15 mg achieved 20.2% weight loss versus 13.7% for semaglutide 2.4 mg - a statistically significant 6.5 percentage point advantage for tirzepatide.
What Drives the Differences?
Three pharmacological factors primarily explain the weight loss gradient across the class:
1. Receptor engagement breadth. Single GLP-1 agonists work through one receptor. Tirzepatide's dual GIP/GLP-1 engagement accesses complementary appetite circuits and may improve metabolic flexibility. Retatrutide adds glucagon-mediated energy expenditure on top of dual incretin appetite suppression. Each additional receptor pathway contributes incrementally to total caloric deficit.
2. Hypothalamic exposure. Not all GLP-1 agonists penetrate the blood-brain barrier or access circumventricular organs equally. Semaglutide, with its relatively small molecular size and high albumin binding, achieves substantial CNS exposure. Dulaglutide, with its large Fc domain, may have more limited central penetration. This could partially explain why dulaglutide produces less weight loss despite adequate peripheral GLP-1 receptor activation.
3. Gastric emptying effects. All GLP-1 agonists slow gastric emptying, but the degree varies. Semaglutide and exenatide BID produce the most pronounced gastric emptying delay, contributing to early satiety and reduced meal size. This effect attenuates over weeks of treatment (tachyphylaxis), which is why the weight loss curves for GLP-1 agonists typically plateau at 60-72 weeks rather than continuing indefinitely.
REAL-WORLD VS. TRIAL RESULTS
Clinical trials involve rigorous patient selection, regular monitoring, lifestyle counseling, and high adherence rates. Real-world studies consistently show 30-50% lower weight loss than key trial results. A Truveta analysis of electronic health records found real-world weight loss of approximately 5.9% with semaglutide at 12 months, compared to the 14.9% seen in STEP 1. The absolute ranking between drugs still holds in real-world data, but patients should be counseled that their results will likely fall below published trial figures.
Weight Loss Trajectories and Plateaus
An underappreciated aspect of GLP-1 weight loss is the temporal pattern. Weight doesn't decline linearly. Most patients experience rapid weight loss in the first 12-20 weeks during dose escalation, followed by progressively slower loss as the body's counter-regulatory mechanisms engage. Metabolic adaptation - a reduction in resting energy expenditure beyond what's predicted by lost mass - kicks in around 3-6 months and partially offsets the caloric deficit created by reduced appetite.
Peak weight loss is typically reached between 60 and 72 weeks with semaglutide and tirzepatide. After that, weight tends to stabilize. Discontinuation leads to weight regain - the STEP 1 extension trial showed that patients regained approximately two-thirds of lost weight within 1 year of stopping semaglutide. This has made the question of treatment duration a central issue in obesity medicine. Current consensus treats GLP-1 agonists as chronic medications, similar to antihypertensives - you keep taking them to maintain the effect.
For detailed guidance on optimizing weight loss with each agent, visit the GLP-1 weight loss overview or use the dosing calculator to model titration schedules.
HbA1c Reduction Comparison
GLP-1 receptor agonists were developed as diabetes drugs, and glycemic control remains a primary indication for most agents in this class. HbA1c reduction reflects average blood glucose over the preceding 2-3 months and serves as the gold standard for comparing antidiabetic efficacy.
HbA1c Data by Agent
| Drug | Trial | Dose | Baseline HbA1c | HbA1c Change | % Reaching <7.0% |
|---|---|---|---|---|---|
| Exenatide BID | AMIGO-2 | 10 mcg BID | 8.5% | -0.86% | 27% |
| Exenatide QW | DURATION-5 | 2 mg QW | 8.5% | -1.6% | 58% |
| Liraglutide | LEAD-6 | 1.8 mg QD | 8.2% | -1.12% | 54% |
| Dulaglutide | AWARD-1 | 1.5 mg QW | 8.1% | -1.51% | 78% |
| Semaglutide | SUSTAIN-7 | 1.0 mg QW | 8.2% | -1.8% | 67% |
| Tirzepatide | SURPASS-1 | 15 mg QW | 7.9% | -2.07% | 92% |
| Tirzepatide | SURPASS-2 | 15 mg QW | 8.3% | -2.46% | 92% |
What These Numbers Mean in Practice
The American Diabetes Association generally recommends an HbA1c target of less than 7.0% for most adults with diabetes. Looking at the table above, the percentage of patients achieving this target varies enormously: from 27% with exenatide BID to 92% with tirzepatide 15 mg. In SURPASS-2, tirzepatide brought 51% of patients below an HbA1c of 5.7% - the threshold for normal glucose tolerance. Some researchers describe this as pharmacological diabetes remission, though the term remains debated.
Semaglutide 1.0 mg sits firmly in the middle of the pack for glycemic control, producing consistent HbA1c reductions of 1.5-1.8% across the SUSTAIN trials. When SURPASS-2 compared tirzepatide head-to-head with semaglutide 1.0 mg, all three tirzepatide doses (5 mg, 10 mg, 15 mg) produced statistically superior HbA1c reductions. The 15 mg dose achieved a 0.6% greater HbA1c reduction than semaglutide - a clinically meaningful margin.
Mechanisms of Glycemic Superiority
Why does tirzepatide outperform pure GLP-1 agonists for glucose control? The GIP component provides additive insulinotropic effects through a distinct receptor signaling cascade. While GLP-1 and GIP both increase intracellular cAMP in beta cells, they do so through different downstream effectors. The combined stimulation produces more strong first-phase insulin secretion - the initial spike of insulin within 10-15 minutes of glucose exposure that is characteristically blunted in type 2 diabetes.
GIP agonism also appears to improve beta cell function and survival through trophic effects that are independent of and complementary to GLP-1 signaling. Animal studies show that dual incretin stimulation promotes beta cell proliferation and inhibits apoptosis more effectively than either agonist alone. Whether this translates to durable remission of type 2 diabetes in humans is an active area of investigation.
The weight loss itself contributes meaningfully to glycemic improvement. Every 1% of body weight lost is associated with approximately a 0.1% reduction in HbA1c, though this relationship is non-linear and more pronounced in patients with higher baseline HbA1c values. Given that tirzepatide produces 6-7% more weight loss than semaglutide 1.0 mg, the incremental weight loss alone could account for roughly 0.3-0.5% of the HbA1c difference between the two drugs.
CLINICAL PEARL
For patients with type 2 diabetes who are already on a GLP-1 agonist but haven't reached target HbA1c, switching from a single GLP-1 agonist to tirzepatide offers a meaningful step-up in glycemic efficacy. The SURPASS-4 trial showed that tirzepatide was superior to insulin glargine (mean dose 44 units/day) for HbA1c reduction, while also producing weight loss instead of the weight gain typical with insulin therapy. For the right patient, dual incretin therapy can replace or defer insulin initiation.
Oral Semaglutide: A Special Case
Oral semaglutide (Rybelsus) deserves separate mention. At the currently approved 14 mg dose, HbA1c reductions range from 0.9-1.3% in the PIONEER trial program - measurably less than injectable semaglutide at 1.0 mg. This reflects the low oral bioavailability (approximately 1%) and the practical challenges of consistent absorption.
The PIONEER PLUS study tested higher oral doses (25 mg and 50 mg) and found HbA1c reductions of 1.5-1.8% - comparable to injectable semaglutide 1.0 mg. A higher-dose oral semaglutide formulation is under regulatory review and could close the efficacy gap between oral and injectable formulations. See the orforglipron guide for coverage of next-generation oral GLP-1 approaches that may solve the bioavailability problem entirely.
Cardiovascular Outcomes Across the Class

Cardiovascular disease is the leading cause of death in patients with type 2 diabetes and a major comorbidity in obesity. The cardiovascular outcomes trials (CVOTs) for GLP-1 agonists have arguably generated more excitement among cardiologists than endocrinologists, because they demonstrate risk reduction beyond what glucose lowering alone would predict.
Cardiovascular Outcomes Trial Results
| Trial | Drug | N | Population | Median Follow-up | MACE HR (95% CI) | Result |
|---|---|---|---|---|---|---|
| ELIXA (2015) | Lixisenatide 20 mcg | 6,068 | T2DM + recent ACS | 2.1 yr | 1.02 (0.89-1.17) | Non-inferior |
| LEADER (2016) | Liraglutide 1.8 mg | 9,340 | T2DM + high CV risk | 3.8 yr | 0.87 (0.78-0.97) | Superior |
| SUSTAIN-6 (2016) | Semaglutide 0.5/1.0 mg | 3,297 | T2DM + high CV risk | 2.1 yr | 0.74 (0.58-0.95) | Superior |
| EXSCEL (2017) | Exenatide QW 2 mg | 14,752 | T2DM +/- CVD | 3.2 yr | 0.91 (0.83-1.00) | Non-inferior |
| HARMONY (2018) | Albiglutide 30-50 mg | 9,463 | T2DM + CVD | 1.6 yr | 0.78 (0.68-0.90) | Superior |
| REWIND (2019) | Dulaglutide 1.5 mg | 9,901 | T2DM + CV risk factors | 5.4 yr | 0.88 (0.79-0.99) | Superior |
| PIONEER 6 (2019) | Oral sema 14 mg | 3,183 | T2DM + high CV risk | 1.3 yr | 0.79 (0.57-1.11) | Non-inferior |
| SELECT (2023) | Semaglutide 2.4 mg | 17,604 | Obesity + CVD, no T2DM | 3.4 yr | 0.80 (0.72-0.90) | Superior |
Interpreting the CVOT Landscape
The pattern across these trials tells a consistent story: GLP-1 receptor agonists as a class reduce cardiovascular risk, with the magnitude of benefit varying by agent and population. Four key observations emerge:
1. Longer-acting agents show clearer benefit. Liraglutide, semaglutide, dulaglutide, and albiglutide all demonstrated CV superiority. Exenatide QW narrowly missed (upper CI bound of exactly 1.00), while lixisenatide (the shortest-acting agent, with a 3-hour half-life) showed no benefit. One hypothesis is that sustained GLP-1 receptor activation, rather than intermittent stimulation, is required for cardioprotection.
2. SELECT changed the paradigm. Before SELECT, GLP-1 CV benefit was demonstrated only in patients with type 2 diabetes. SELECT enrolled patients with obesity and established cardiovascular disease but excluded those with diabetes. The 20% MACE reduction proved that semaglutide's cardiovascular protection is independent of glucose lowering. This expanded the indication framework from "diabetes drug with CV benefit" to "cardiovascular drug that also treats diabetes and obesity."
3. The benefit is driven primarily by atherosclerotic events. Across trials, the MACE reduction comes predominantly from reductions in non-fatal myocardial infarction and non-fatal stroke, with less consistent effects on cardiovascular death. This is consistent with an anti-atherosclerotic mechanism - likely mediated by reductions in inflammation (CRP decreases of 20-40%), blood pressure (2-5 mmHg systolic), atherogenic lipoproteins, and body weight.
4. Heart failure data is emerging. The STEP-HFpEF trial showed that semaglutide 2.4 mg improved symptoms, physical limitations, and exercise function in patients with heart failure with preserved ejection fraction (HFpEF) and obesity. This extends the cardiovascular indication beyond atherosclerotic disease to a condition with few effective treatments.
WHAT ABOUT TIRZEPATIDE?
Tirzepatide's cardiovascular outcomes trial (SURPASS-CVOT) is ongoing and expected to report results in late 2027. Pre-specified analyses from SURMOUNT and SURPASS trials show favorable trends in cardiovascular risk factors - larger reductions in blood pressure, triglycerides, and CRP than semaglutide. Many cardiologists expect tirzepatide to demonstrate CV benefit, but until SURPASS-CVOT reports, semaglutide remains the only GLP-1 agonist with proven cardiovascular benefit in patients without diabetes.
Beyond MACE: Renal and Hepatic Outcomes
The FLOW trial (2024) demonstrated that semaglutide 1.0 mg reduced the risk of kidney disease progression by 24% in patients with type 2 diabetes and chronic kidney disease. This was the first dedicated renal outcomes trial for a GLP-1 agonist and established a new indication for the class.
Hepatic outcomes are equally promising. GLP-1 agonists reduce liver fat content, and the GLP-1/glucagon dual agonist survodutide has shown particular efficacy for metabolic dysfunction-associated steatohepatitis (MASH), with histological improvement in over 60% of patients in Phase 2 trials. Semaglutide is also being studied in the ESSENCE trial for MASH, with results expected in 2026.
Side Effect Comparison
The side effect profile of GLP-1 agonists is dominated by gastrointestinal symptoms - nausea, vomiting, diarrhea, and constipation. These effects are mechanism-based, arising from the same receptor activation that produces therapeutic benefit. The clinical question isn't whether GI side effects occur, but how frequent and severe they are across drugs, and how they can be managed.
GI Side Effect Rates by Agent
| Drug / Dose | Nausea | Vomiting | Diarrhea | Constipation | Discontinuation (GI) |
|---|---|---|---|---|---|
| Exenatide 10 mcg BID | 20% | 10% | 12% | 6% | 4% |
| Liraglutide 1.8 mg QD | 24% | 8% | 11% | 8% | 5% |
| Liraglutide 3.0 mg QD | 39% | 15% | 20% | 12% | 7% |
| Dulaglutide 1.5 mg QW | 12% | 5% | 9% | 4% | 2% |
| Dulaglutide 4.5 mg QW | 15% | 7% | 10% | 5% | 3% |
| Semaglutide 1.0 mg QW | 20% | 5% | 9% | 5% | 4% |
| Semaglutide 2.4 mg QW | 44% | 25% | 30% | 24% | 7% |
| Tirzepatide 5 mg QW | 18% | 5% | 12% | 6% | 3% |
| Tirzepatide 10 mg QW | 22% | 8% | 13% | 7% | 4% |
| Tirzepatide 15 mg QW | 26% | 10% | 17% | 11% | 5% |
Key Patterns in the Side Effect Data
Dose dependence is universal. Every agent shows higher GI side effect rates at higher doses. Semaglutide 2.4 mg (the obesity dose) has nearly double the nausea rate of semaglutide 1.0 mg (the standard diabetes dose). This is why slow, stepwise dose escalation is critical - it allows GI tolerance to develop before reaching the full therapeutic dose.
Dulaglutide is the best tolerated. Across comparable doses, dulaglutide consistently shows the lowest nausea and vomiting rates. The 12-15% nausea incidence at the 1.5-4.5 mg doses is roughly half what's seen with equivalent doses of semaglutide or liraglutide. The tradeoff is lower weight loss efficacy. There is something of an inverse relationship between GI side effects and weight loss across the class - the drugs that cause more nausea tend to produce more weight loss.
Tirzepatide's GI profile is better than its weight loss would predict. Given that tirzepatide produces more weight loss than semaglutide 2.4 mg, you might expect worse GI side effects. But tirzepatide 15 mg has a nausea rate of 26% versus semaglutide 2.4 mg's 44%. This favorable ratio may reflect the GIP component's dampening effect on area postrema activation, as discussed in the incretin biology section.
Serious and Rare Adverse Events
Beyond the common GI effects, several serious adverse events warrant discussion:
Pancreatitis: All GLP-1 agonist labels carry a warning about acute pancreatitis. The absolute risk increase is small - approximately 0.1-0.3% across key trials, compared to 0.1-0.2% for placebo. Large observational studies and meta-analyses have not confirmed a clinically significant increase in pancreatitis risk. Still, GLP-1 agonists should be discontinued in any patient with confirmed pancreatitis, and they're contraindicated in patients with a history of pancreatitis.
Thyroid C-cell tumors: In rodent studies, GLP-1 agonists cause dose-dependent increases in thyroid C-cell hyperplasia and medullary thyroid carcinoma (MTC). This is likely rodent-specific - human thyroid C-cells express far fewer GLP-1 receptors than rodent C-cells. No increased MTC risk has been observed in human clinical trials or post-marketing surveillance spanning over 15 years. Nevertheless, all GLP-1 agonists carry a boxed warning and are contraindicated in patients with a personal or family history of MTC or multiple endocrine neoplasia syndrome type 2 (MEN2).
Gallbladder events: Rapid weight loss from any cause increases the risk of gallstones. GLP-1 agonist trials have shown a modest increase in cholelithiasis and cholecystitis. In STEP 1, gallbladder events occurred in 2.6% of semaglutide patients versus 1.2% on placebo. Patients losing more than 1.5 kg per week during initial treatment may benefit from prophylactic ursodiol, though this isn't standard practice yet.
Gastroparesis concerns: GLP-1 agonists slow gastric emptying, which has raised theoretical concerns about worsening gastroparesis. Patients with pre-existing gastroparesis should use GLP-1 agonists cautiously. There have also been anecdotal reports of retained gastric contents in patients undergoing anesthesia while on GLP-1 therapy, prompting the American Society of Anesthesiologists to recommend holding GLP-1 agonists before elective procedures requiring sedation.
Muscle loss: Weight loss from GLP-1 agonists includes both fat and lean mass. In STEP 1, approximately 39% of total weight lost was lean mass (including muscle). This has led to concerns about sarcopenia, particularly in older patients. Resistance training and adequate protein intake (1.2-1.6 g/kg/day) during GLP-1 therapy are strongly recommended to preserve muscle mass. Adding tesofensine or other agents that preferentially target fat loss is an area of active investigation.
MANAGING GI SIDE EFFECTS
The most effective strategy is slow dose escalation - following the prescribed titration schedule and not advancing the dose until GI symptoms from the current dose have resolved. Eating smaller meals, avoiding high-fat foods, and staying hydrated all help. For persistent nausea, ondansetron (Zofran) 4-8 mg as needed is commonly prescribed off-label. Ginger supplements and vitamin B6 may provide mild relief. If GI symptoms remain intolerable at the target dose, dose reduction (with acceptance of less weight loss) is preferable to discontinuation.
Dosing & Administration Comparison
Dosing convenience has been a major driver of adoption across the GLP-1 class. The evolution from twice-daily injections to once-weekly formulations - and now oral options - has dramatically improved adherence. Here's exactly how each agent is dosed, titrated, and administered.
Complete Titration Schedules
| Drug | Starting Dose | Titration Steps | Target Dose | Time to Target |
|---|---|---|---|---|
| Exenatide BID (Byetta) | 5 mcg BID | 5 mcg BID x 4 wk, then 10 mcg BID | 10 mcg BID | 4 weeks |
| Exenatide QW (Bydureon) | 2 mg QW | No titration needed | 2 mg QW | Immediate |
| Liraglutide (Victoza) | 0.6 mg QD | 0.6 mg x 1 wk, 1.2 mg x 1 wk, 1.8 mg | 1.8 mg QD | 2-3 weeks |
| Liraglutide (Saxenda) | 0.6 mg QD | 0.6 mg increments weekly | 3.0 mg QD | 5 weeks |
| Dulaglutide (Trulicity) | 0.75 mg QW | 0.75 mg x 4 wk, then 1.5 mg; may increase to 3.0 or 4.5 mg | 1.5-4.5 mg QW | 4-12 weeks |
| Semaglutide (Ozempic) | 0.25 mg QW | 0.25 mg x 4 wk, 0.5 mg x 4 wk, 1.0 mg; optional 2.0 mg | 1.0-2.0 mg QW | 8-16 weeks |
| Semaglutide (Wegovy) | 0.25 mg QW | 0.25, 0.5, 1.0, 1.7 mg (4 wk each), then 2.4 mg | 2.4 mg QW | 16-20 weeks |
| Oral semaglutide (Rybelsus) | 3 mg QD | 3 mg x 30 days, 7 mg x 30 days, 14 mg | 14 mg QD | 8 weeks |
| Tirzepatide (Mounjaro/Zepbound) | 2.5 mg QW | 2.5 mg x 4 wk, then 5 mg; increase by 2.5 mg q4wk | 5-15 mg QW | 4-24 weeks |
Administration Details
Injectable formulations: All injectable GLP-1 agonists are administered subcutaneously in the abdomen, thigh, or upper arm. Most modern formulations come in pre-filled, single-use or multi-dose pens with hidden needles and automatic injection mechanisms. Needle gauge is typically 31-32G (very fine). Injection site rotation is recommended to prevent lipodystrophy, though this is uncommon with GLP-1 agonists compared to insulin.
Oral semaglutide (Rybelsus): Must be taken on an empty stomach with no more than 4 oz (120 mL) of plain water. Wait at least 30 minutes before eating, drinking, or taking other oral medications. The SNAC absorption enhancer creates a transient local pH change in the gastric mucosa that facilitates transcellular peptide absorption. Food, larger water volumes, or other medications in the stomach dramatically reduce bioavailability.
Exenatide QW (Bydureon): The microsphere formulation requires reconstitution before injection - the patient mixes the powder with the diluent by tapping and rolling the vial. This is a unique administration burden not shared by other agents and contributed to Bydureon's commercial underperformance.
Switching Between Agents
Switching from one GLP-1 agonist to another is common in clinical practice, whether due to inadequate efficacy, intolerable side effects, insurance changes, or the desire to try a newer agent. General guidance for switching:
- Same-day switch for weekly agents: When switching between once-weekly agents (e.g., semaglutide to tirzepatide), administer the first dose of the new agent on the day the next dose of the old agent would have been due. Start at the beginning dose of the new agent and titrate per label.
- Daily to weekly: When switching from liraglutide (daily) to a once-weekly agent, discontinue liraglutide and start the weekly agent the next day. Begin at the starting dose.
- GI tolerance doesn't transfer: Tolerance to GI side effects developed on one GLP-1 agonist does not reliably carry over to another. Patients switching agents should be warned that nausea may recur during the titration period of the new drug.
- No washout needed: There is no required washout period between agents. The pharmacological overlap during switching is not clinically problematic.
For personalized titration guidance, the FormBlends dosing calculator can model schedule options for each agent. Patients starting therapy can also begin with a free assessment to determine which agent and starting dose may be most appropriate.
Cost & Insurance Comparison

Cost is the single biggest barrier to GLP-1 agonist access. US list prices range from $800 to $1,600 per month, and insurance coverage remains inconsistent - particularly for the obesity indication. Understanding the full pricing landscape, including manufacturer coupons, insurance tiers, and compounding alternatives, is essential for patients and prescribers navigating this market.
US List Prices (Early 2026)
| Drug | Brand | Indication | Monthly List Price | Annual List Price |
|---|---|---|---|---|
| Exenatide BID | Byetta | T2DM | ~$800 | ~$9,600 |
| Exenatide QW | Bydureon BCise | T2DM | ~$850 | ~$10,200 |
| Liraglutide | Victoza | T2DM | ~$1,200 | ~$14,400 |
| Liraglutide | Saxenda | Obesity | ~$1,400 | ~$16,800 |
| Dulaglutide | Trulicity | T2DM | ~$950 | ~$11,400 |
| Semaglutide | Ozempic | T2DM | ~$1,000 | ~$12,000 |
| Semaglutide | Wegovy | Obesity | ~$1,350 | ~$16,200 |
| Oral semaglutide | Rybelsus | T2DM | ~$1,000 | ~$12,000 |
| Tirzepatide | Mounjaro | T2DM | ~$1,100 | ~$13,200 |
| Tirzepatide | Zepbound | Obesity | ~$1,060 | ~$12,720 |
These are wholesale acquisition costs (WAC) and represent the list price before rebates, discounts, or insurance negotiations. What patients actually pay depends entirely on their coverage situation.
Insurance Coverage Landscape
Diabetes indication: Most commercial insurance plans and Medicare Part D cover at least one GLP-1 agonist for type 2 diabetes. Preferred agents vary by plan - some favor Ozempic, others Trulicity or Mounjaro. Prior authorization is nearly universal, typically requiring documented failure of metformin or other first-line agents. With insurance, copays for diabetes-indicated GLP-1 agonists typically range from $25 to $150 per month.
Obesity indication: Coverage is far less consistent. Medicare explicitly excludes weight loss medications from Part D coverage by statute. Many commercial plans also exclude obesity drugs or impose stringent criteria (BMI thresholds, documented comorbidities, supervised diet failure). Even when covered, obesity-indicated drugs often sit on higher formulary tiers with copays of $150 to $500 per month.
Employer plans: Self-insured employers are increasingly adding GLP-1 coverage for obesity, driven by data showing that treated employees have lower healthcare costs over 3-5 year horizons. But some employers have removed coverage due to short-term cost concerns - the annual per-patient cost of $12,000-16,000 multiplied across an employee population creates significant budget impact.
Manufacturer Savings Programs
Both Novo Nordisk and Eli Lilly offer manufacturer savings cards that reduce out-of-pocket costs for commercially insured patients. These programs typically bring copays down to $25 per month for eligible patients. They do not apply to government-insured patients (Medicare, Medicaid, Tricare) due to federal anti-kickback regulations.
Eli Lilly introduced LillyDirect, which offers Zepbound at $399 per month for cash-pay patients without insurance coverage - a 60% discount from list price. Novo Nordisk has similar direct-to-patient programs. These programs represent a meaningful cost reduction but still place the annual cost at approximately $4,800 - a significant expense for many patients.
Compounded GLP-1 Formulations
During the FDA-recognized shortage of semaglutide and tirzepatide (2022-2025), 503A and 503B compounding pharmacies were permitted to produce compounded versions of these peptides. Compounded semaglutide and tirzepatide have been available at significantly lower costs - typically $200 to $500 per month depending on dose and provider.
Providers like FormBlends offer compounded formulations with physician oversight, dosing guidance, and quality-controlled sourcing. For patients without insurance coverage for brand-name products, compounded formulations have expanded access to a treatment class that would otherwise be financially unreachable. The regulatory landscape around compounding continues to evolve, and patients should work with reputable providers that use cGMP-compliant 503B outsourcing facilities.
COST-EFFECTIVENESS PERSPECTIVE
Multiple health economic analyses have found GLP-1 agonists to be cost-effective for type 2 diabetes when factoring in reduced cardiovascular events, hospitalizations, and long-term complications. For obesity, cost-effectiveness is more debated - it depends heavily on the duration of treatment, the magnitude of sustained weight loss, and whether downstream health savings (fewer joint replacements, less sleep apnea treatment, reduced cancer incidence) materialize over 10-20 year horizons. The Institute for Clinical and Economic Review (ICER) estimated a cost-effective price of approximately $7,500 per year for GLP-1 agonists in obesity - roughly half the current list price.
Pipeline: Next-Generation Agents
The GLP-1 pipeline is the most active area of pharmaceutical development in the world right now. Over a dozen novel molecules are in Phase 2 or Phase 3 trials, each attempting to improve on current agents in one or more dimensions: greater weight loss, fewer side effects, oral delivery, longer dosing intervals, or new therapeutic indications.
Retatrutide (Eli Lilly) - Triple GLP-1/GIP/Glucagon Agonist
Retatrutide is the most anticipated pipeline compound. Its Phase 2 trial (Jastreboff et al., NEJM 2023) reported 24.2% mean body weight reduction at the 12 mg dose over 48 weeks - the highest weight loss ever recorded for any anti-obesity medication. At this level of weight loss, the results approach those of bariatric surgery procedures like sleeve gastrectomy.
The triple agonist mechanism combines appetite suppression (GLP-1 + GIP) with increased energy expenditure (glucagon). Phase 3 trials (TRIUMPH program) are underway for both obesity and type 2 diabetes, with results expected in 2026-2027. If the Phase 3 data confirms Phase 2 findings, retatrutide could become the most effective pharmaceutical weight loss treatment available.
Key questions remain around the glucagon component: will it cause hepatic steatosis rebound if discontinued? Could the increased energy expenditure lead to excessive lean mass loss? And what is the long-term cardiovascular safety profile of chronic glucagon receptor activation? The Phase 3 program is designed to answer these. See the retatrutide complete guide for detailed analysis.
Orforglipron (Eli Lilly) - Oral Non-Peptide GLP-1 Agonist
Orforglipron represents a fundamentally different approach. Rather than a peptide that must be protected from digestive enzymes, orforglipron is a small-molecule GLP-1 receptor agonist - the first of its kind to reach late-stage development. As a non-peptide, it has high oral bioavailability without the fasting and water restrictions that limit oral semaglutide (Rybelsus).
Phase 2 results showed weight loss of up to 14.7% at 36 weeks and HbA1c reductions of up to 2.1%. The GI side effect profile was comparable to injectable GLP-1 agonists. Phase 3 trials (ATTAIN program) are ongoing for both obesity and type 2 diabetes.
If approved, orforglipron could fundamentally change the market by offering a convenient daily pill with efficacy approaching injectable semaglutide. For the millions of patients who refuse or cannot tolerate injections, this would be transformative. The projected price point is also expected to be lower than injectable formulations, given simpler manufacturing.
Survodutide (Boehringer Ingelheim/Zealand) - GLP-1/Glucagon Dual Agonist
Survodutide activates both GLP-1 and glucagon receptors, but unlike retatrutide, it does not include GIP agonism. Phase 2 data showed weight loss of up to 18.7% at 46 weeks in patients with obesity and up to 19% in those with MASH. The MASH data is particularly compelling - survodutide achieved MASH resolution without worsening fibrosis in over 60% of patients, likely driven by glucagon's hepatic lipid-mobilizing effects.
Phase 3 trials are underway for both obesity (SYNCHRONIZE program) and MASH (ACHIEVE program). Survodutide may carve out a niche as the preferred agent for patients with obesity-associated fatty liver disease.
CagriSema (Novo Nordisk) - Cagrilintide + Semaglutide
CagriSema combines cagrilintide (a long-acting amylin analog) with semaglutide in a single once-weekly injection. The REDEFINE Phase 3 program showed weight loss of up to 22.7% at 68 weeks. The amylin component adds a complementary appetite-suppression pathway through the area postrema and hypothalamus, targeting different neuronal populations than GLP-1.
Amylin, co-secreted with insulin from beta cells, slows gastric emptying and suppresses glucagon secretion through mechanisms distinct from GLP-1. The combination approach essentially layers two appetite-suppression signals on top of each other. CagriSema is expected to be submitted for regulatory approval by Novo Nordisk in 2026.
Other Pipeline Agents
| Compound | Company | Mechanism | Phase | Key Data |
|---|---|---|---|---|
| Pemvidutide | Altimmune | GLP-1/glucagon dual | Phase 2 | ~15% weight loss at 48 wk; strong liver fat reduction |
| Maritide (MariTide) | Amgen | GIP antagonist/GLP-1 agonist + anti-GIPR antibody | Phase 2 | ~14% weight loss at 12 wk; monthly dosing potential |
| Danuglipron | Pfizer | Oral small-molecule GLP-1 | Phase 2b (modified) | Troubled development; reformulated for twice-daily dosing |
| Ecnoglutide | Sciwind Biosciences | GLP-1 agonist (long-acting) | Phase 3 (China) | Biweekly dosing; ~17% weight loss at 48 wk |
| Mazdutide | Innovent Biologics | GLP-1/glucagon dual | Phase 3 | Approved in China (2024); ~16% weight loss |
| Amycretin | Novo Nordisk | Amylin/GLP-1 dual oral | Phase 2 | ~13% weight loss at 12 wk (oral formulation) |
The sheer volume of pipeline activity ensures that the current generation of approved GLP-1 agonists will face competition from multiple directions within 2-3 years. Oral formulations, longer dosing intervals, and combined mechanisms will likely drive the next wave of market share shifts. For ongoing coverage, follow our GLP-1 research hub.
Patient Selection and Clinical Decision-Making Across the GLP-1 Class
With multiple GLP-1 receptor agonists now available, each with distinct efficacy profiles, side effect patterns, dosing schedules, and costs, the clinical challenge has shifted from "should we prescribe a GLP-1?" to "which GLP-1 is right for this particular patient?" This section provides a systematic framework for matching individual patient characteristics to specific agents within the class.
The Primary Goal Framework
The first decision point is identifying the patient's primary therapeutic goal, which typically falls into one of four categories: maximum weight loss, optimal glycemic control, cardiovascular risk reduction, or a balanced approach addressing multiple goals simultaneously. While all GLP-1 agonists provide some benefit across all these domains, the degree of benefit varies substantially by agent, and choosing the best-matched drug can significantly improve outcomes.
For patients whose primary goal is maximum weight loss, the evidence hierarchy is clear: tirzepatide at the 15 mg dose produces the greatest weight reduction (approximately 21% in SURMOUNT-1), followed by semaglutide 2.4 mg (approximately 15% in STEP 1), then liraglutide 3.0 mg (approximately 8% in SCALE), then dulaglutide 4.5 mg and exenatide ER. Among pipeline agents, retatrutide has shown approximately 24% weight loss at the highest dose, potentially becoming the most effective single agent once approved.
For patients whose primary goal is glycemic control in Type 2 diabetes, the ranking shifts somewhat. Tirzepatide still leads with approximately 2.3% HbA1c reduction at the 15 mg dose, but injectable semaglutide 1.0 mg (approximately 1.8% reduction) and dulaglutide 4.5 mg (approximately 1.7% reduction) are closer in glycemic efficacy than in weight loss efficacy. For patients with more moderate glycemic needs (HbA1c 7-8%), oral semaglutide (Rybelsus) at 14 mg provides approximately 1.4% HbA1c reduction with the convenience of oral administration.
For patients whose primary goal is cardiovascular risk reduction, the evidence base favors drugs with completed cardiovascular outcomes trials (CVOTs) showing MACE reduction. Semaglutide has the strongest CV evidence through the SELECT trial (20% MACE reduction in patients with CVD but without diabetes) and the SUSTAIN-6 trial (26% MACE reduction in diabetic patients). Liraglutide demonstrated 13% MACE reduction in the LEADER trial. Dulaglutide showed non-inferiority but not superiority in REWIND. Tirzepatide's CVOT (SURPASS-CVOT) is still ongoing. For patients with established cardiovascular disease, choosing a GLP-1 with proven CV benefit is an evidence-based imperative.
Side Effect Tolerance and Management
All GLP-1 receptor agonists produce gastrointestinal side effects (nausea, vomiting, diarrhea, constipation), but the severity and pattern vary by agent and formulation. Nausea rates range from approximately 20% with liraglutide to approximately 44% with semaglutide 2.4 mg in key trials. However, several factors affect real-world tolerability beyond headline rates.
The titration schedule is perhaps the most important determinant of GI tolerability. Semaglutide uses a 16-week titration from 0.25 mg to 2.4 mg, while tirzepatide uses a 20-week titration from 2.5 mg to 15 mg. Patients who experience significant nausea during titration can extend the time at each dose step, reducing nausea severity at the cost of a slower onset of full therapeutic effect. Patients with a history of gastroparesis, cyclic vomiting syndrome, or severe GI sensitivity should start with the longest available titration schedule and advance doses only when fully tolerating the current dose.
For patients who have tried one GLP-1 agonist and experienced intolerable GI side effects, switching to a different agent within the class sometimes improves tolerability. The mechanism isn't fully understood, but differences in receptor binding kinetics, tissue distribution, and half-life between agents may create different GI stimulation patterns. A patient who couldn't tolerate semaglutide's weekly dosing pattern might do better with daily liraglutide (which produces more consistent but lower peak drug levels) or with tirzepatide (which engages both GLP-1 and GIP receptors, potentially modifying the GI stimulation profile).
Dosing Frequency Preferences
Patient preference for dosing frequency is a practical consideration that significantly affects long-term adherence. Weekly injectable options (semaglutide, tirzepatide, dulaglutide, exenatide ER) are generally preferred over daily injectables (liraglutide, exenatide BID) because they require fewer injection events and create less daily treatment burden. Among weekly options, the choice often comes down to device preference and tolerability.
For patients who strongly prefer oral medication over injections, oral semaglutide (Rybelsus) provides a non-injectable option, though with somewhat lower weight loss efficacy than injectable semaglutide (approximately 7-9% versus 15% body weight loss). The oral formulation requires specific administration conditions (30 minutes before food, with a small amount of plain water, no other medications within 30 minutes) that some patients find cumbersome. Pipeline oral agents like orforglipron (a non-peptide oral GLP-1 agonist) may provide oral options with efficacy closer to injectable formulations.
For patients who prefer the least possible treatment burden, monthly or longer-acting depot formulations are in development. These ultra-long-acting formulations could reduce injection frequency to 12 or fewer per year, potentially improving adherence for patients who struggle with weekly injection schedules. Until these become available, tirzepatide and semaglutide weekly injections using autoinjector pens represent the current best balance of efficacy and convenience.
Special Population Considerations
Renal impairment affects drug selection within the GLP-1 class. While GLP-1 agonists are not renally cleared (they are proteolytically degraded), renal function affects comorbidity management and overall risk. Semaglutide has the most extensive renal safety data through the FLOW trial, which demonstrated 24% reduction in kidney disease progression in patients with Type 2 diabetes and chronic kidney disease. For patients with significant renal impairment (eGFR below 30 mL/min), semaglutide is the best-supported choice within the class.
Hepatic considerations are also relevant. Patients with MASLD/NASH may benefit preferentially from semaglutide (which has Phase 3 data from the ESSENCE trial showing steatohepatitis resolution in 62% of patients) or from tirzepatide (which has shown similar hepatic benefits in the Combined effect-NASH trial). The liver-protective effects appear to be mediated by both weight loss and direct hepatic GLP-1 receptor activation, making GLP-1 agonists uniquely suited for patients with metabolic liver disease.
Age-related considerations influence drug selection as well. Elderly patients (over 65) are at higher risk for the lean mass loss that accompanies GLP-1-induced weight loss, and for these patients, slower titration, lower maximum doses, and concurrent resistance training are particularly important. Growth hormone secretagogues like CJC-1295/Ipamorelin or sermorelin may support lean mass preservation in elderly patients on GLP-1 therapy, though this combination hasn't been studied in clinical trials.
Mechanism Deep-Dive: How Each GLP-1 Agent Differs at the Molecular Level
Understanding the molecular differences between GLP-1 agents explains why drugs that all target the same receptor produce meaningfully different clinical outcomes. The differences aren't just about dose and half-life; they reflect fundamental variations in receptor interaction, signaling bias, tissue distribution, and multi-target engagement that create distinct pharmacological profiles.
Receptor Binding Kinetics and Signaling Bias
GLP-1 receptors signal through multiple intracellular pathways, including Gs-mediated cAMP production, beta-arrestin recruitment, and receptor internalization. Different GLP-1 agonists activate these pathways in different proportions, a phenomenon called "signaling bias." Semaglutide, for example, shows strong Gs/cAMP signaling with relatively less beta-arrestin recruitment compared to the native GLP-1 peptide. This bias may contribute to its potent insulin secretagogue effect while producing less receptor downregulation than agents with stronger beta-arrestin signaling.
Exenatide (derived from exendin-4, the Gila monster peptide) has a distinct binding mode compared to human GLP-1-derived analogs. Exendin-4 occupies the GLP-1 receptor in a slightly different orientation, engaging additional contacts in the receptor's extracellular domain. This different binding mode produces a different signaling profile and may explain some of the clinical differences between exenatide-based and human GLP-1-based drugs, despite acting on the same receptor.
Tirzepatide presents an entirely different molecular scenario because it simultaneously engages two distinct receptor systems: GLP-1R and GIPR (glucose-dependent insulinotropic polypeptide receptor). The relative potency at each receptor (approximately 5-fold more potent at GIPR than GLP-1R in vitro) creates a signaling profile that neither a pure GLP-1 agonist nor a pure GIP agonist can replicate. The GIP receptor activation enhances insulin secretion through a pathway complementary to GLP-1, contributes to fat mobilization through adipocyte GIPR signaling, and may have direct CNS appetite-suppressive effects through GIPR in the hypothalamus.
Albumin Binding and Pharmacokinetic Engineering
The long half-lives of modern GLP-1 agonists are achieved primarily through engineered albumin binding. Both semaglutide and liraglutide contain fatty acid side chains (a C18 fatty diacid for semaglutide, a C16 fatty acid for liraglutide) that bind non-covalently to serum albumin. This albumin binding serves three purposes: protecting the peptide from DPP-4 enzymatic degradation, reducing renal clearance (albumin is too large for glomerular filtration), and creating a circulating reservoir that slowly releases free drug as the albumin-bound fraction equilibrates.
The difference in fatty acid chain length between semaglutide and liraglutide is directly responsible for their different half-lives. Semaglutide's C18 diacid binds albumin more tightly (higher binding affinity, slower dissociation rate) than liraglutide's C16 acid, resulting in a half-life of approximately 7 days versus approximately 13 hours. This single molecular modification, the addition of two carbon atoms to the fatty acid chain, transforms a daily injection into a weekly injection and is one of the most elegant examples of pharmacokinetic engineering in modern drug development.
Dulaglutide takes a different approach to half-life extension: it's a fusion protein linking a modified GLP-1 analog to an immunoglobulin Fc fragment. The Fc fusion prevents renal clearance (the molecule is too large for filtration) and allows FcRn-mediated recycling (the neonatal Fc receptor rescues the protein from lysosomal degradation, returning it to the circulation). This produces a half-life of approximately 5 days, sufficient for weekly dosing but shorter than semaglutide's 7-day half-life.
CNS Penetration and Central Appetite Effects
A critical distinction between GLP-1 agonists is their ability to cross the blood-brain barrier (BBB) and directly engage GLP-1 receptors in the hypothalamus, brainstem, and reward circuitry. Native GLP-1, with its 2-minute half-life, has limited CNS penetration. But longer-acting analogs achieve meaningful brain concentrations through several mechanisms: passive diffusion across circumventricular organs (brain regions with incomplete BBB), active transport through the BBB, and signaling through vagal afferents that doesn't require brain penetration at all.
Semaglutide appears to have the highest CNS penetration among approved GLP-1 agonists, which may explain its superior weight loss efficacy relative to drugs with comparable GLP-1 receptor affinity. PET imaging studies using radiolabeled semaglutide have shown accumulation in several brain regions including the hypothalamus, nucleus accumbens, and amygdala - areas involved in appetite regulation, food reward, and emotional responses to food. This central distribution correlates with semaglutide's ability to reduce food noise, cravings, and compulsive eating behaviors to a greater degree than older GLP-1 agonists with less CNS penetration.
Tirzepatide's CNS effects are more complex because both GLP-1R and GIPR are expressed in the brain. The contribution of central GIPR activation to appetite suppression is still being elucidated, but preclinical data suggest that GIPR signaling in the hypothalamus may enhance satiety through mechanisms distinct from GLP-1R signaling, providing additive or complementary appetite suppression. This dual central mechanism could explain tirzepatide's superior weight loss efficacy compared to semaglutide, despite tirzepatide being less potent at GLP-1R alone.
Peripheral Tissue Effects Beyond Pancreas and Brain
GLP-1 receptors are expressed in numerous tissues beyond the pancreas and brain, and different GLP-1 agonists may engage these peripheral receptors to varying degrees, contributing to their distinct clinical profiles. In the heart, GLP-1R activation improves myocardial glucose uptake, reduces inflammation, and may have direct cardioprotective effects during ischemia. In the kidney, GLP-1R activation promotes natriuresis, reduces glomerular hyperfiltration, and has anti-inflammatory effects on podocytes and tubular cells. In the liver, GLP-1R activation reduces de novo lipogenesis, improves hepatic insulin sensitivity, and reduces inflammatory signaling.
The degree to which each GLP-1 agonist engages these peripheral targets depends on its tissue distribution, which is influenced by molecular size, albumin binding, and half-life. Smaller molecules (like exenatide, MW ~4 kDa) penetrate tissues more readily than larger molecules (like dulaglutide, MW ~63 kDa), potentially producing different peripheral effect profiles despite similar receptor affinity. These differences in tissue distribution may contribute to the clinical differences observed between agents in cardiovascular, renal, and hepatic outcomes, beyond what can be explained by differences in weight loss alone.
For patients and providers navigating these molecular complexities, the practical takeaway is that GLP-1 agonists are not interchangeable. Switching between agents within the class should be done with awareness that different drugs may produce different responses in the same patient, not because of "non-response" to the class but because of the distinct pharmacological profiles described above. The comparison hub provides clinical comparison tools that help match individual patient profiles to optimal agents within the GLP-1 class.
Real-World Practice Patterns and Prescribing Trends
Clinical trial data inform prescribing guidelines, but real-world practice patterns reveal how these guidelines are actually implemented and where gaps exist between evidence-based recommendations and clinical reality. Understanding current prescribing patterns provides context for patients navigating the GLP-1 landscape and highlights opportunities for improved care.
Prescribing Volume and Market Dynamics
GLP-1 receptor agonist prescriptions in the United States have grown exponentially, from approximately 5 million prescriptions annually in 2018 to over 45 million in 2025. This growth has been driven primarily by semaglutide (both injectable and oral formulations) and tirzepatide, which together account for over 75% of new GLP-1 prescriptions. The explosive demand has created supply constraints, manufacturing challenges, and price pressures that directly affect patient access.
The prescriber landscape has shifted alongside growing demand. While endocrinologists and diabetes specialists initially dominated GLP-1 prescribing, primary care physicians, obesity medicine specialists, and increasingly, telehealth-based prescribers now write the majority of GLP-1 prescriptions. This democratization of prescribing has improved access for many patients but has also raised concerns about prescribing quality, inadequate titration guidance, and insufficient monitoring of side effects and metabolic parameters.
Adherence Patterns and Discontinuation Rates
Real-world adherence to GLP-1 therapy is substantially lower than in clinical trials. Claims data analyses consistently show that 40-50% of patients discontinue GLP-1 therapy within the first 12 months, compared to less than 10% discontinuation rates in key trials. The most common reasons for real-world discontinuation include cost and insurance coverage changes (approximately 30% of discontinuations), gastrointestinal side effects (approximately 25%), supply shortages and inability to obtain medication (approximately 15%), perceived lack of efficacy (approximately 15%), and decision to try non-pharmacological approaches (approximately 15%).
These discontinuation patterns have important implications for the GLP-1 class comparison. In clinical trials, where adherence is high and monitoring is intensive, the efficacy differences between agents reflect their true pharmacological potential. In the real world, adherence, cost, and access factors may outweigh pharmacological differences in determining which drug produces the best outcomes for a given patient. A theoretically optimal drug that the patient can't afford or can't obtain is less effective than a suboptimal drug that the patient actually takes consistently.
The Compounded GLP-1 Market
Compounded versions of semaglutide and tirzepatide have become a significant component of the GLP-1 market, particularly for patients without insurance coverage or with high copays for brand-name products. Compounding pharmacies like FormBlends provide access to these medications at substantially lower prices, typically $150-350 per month compared to $800-1,350 for brand-name products.
The quality and consistency of compounded GLP-1 medications depend heavily on the pharmacy's manufacturing standards, quality control processes, and regulatory compliance. Pharmacies operating under Section 503B (outsourcing facilities) are subject to FDA inspection and must comply with cGMP requirements, providing a level of quality assurance similar to traditional manufacturers. Section 503A pharmacies (traditional compounding) are regulated primarily by state boards of pharmacy and have less stringent manufacturing requirements, though many maintain high quality standards voluntarily.
For patients considering compounded GLP-1 medications, key quality indicators include third-party potency testing of each batch (confirming that the stated dose matches actual content), sterility testing using USP-compliant methods, endotoxin testing (particularly important for injectable formulations), and beyond-use dating supported by stability studies. The FormBlends science page provides detailed information about quality standards and testing protocols for pharmacy-compounded peptides.
Integration with Lifestyle and Peptide Protocols
In clinical practice, GLP-1 therapy is increasingly prescribed as part of comprehensive metabolic health protocols that include dietary optimization, exercise programming, and sometimes complementary peptide therapy. The rationale for multi-component protocols reflects the understanding that obesity is a multifactorial disease requiring multi-mechanism treatment for optimal outcomes.
Common combinations in clinical practice include GLP-1 therapy plus growth hormone secretagogues (like CJC-1295/Ipamorelin or tesamorelin) for patients concerned about lean mass loss during weight reduction. The GH secretagogue provides anabolic support that counteracts the lean mass-depleting effects of caloric deficit, while the GLP-1 agonist handles appetite suppression and metabolic improvement. This combination hasn't been validated in randomized controlled trials but has strong pharmacological rationale and growing clinical experience.
Other common integrations include GLP-1 therapy plus BPC-157 for patients experiencing GI side effects (BPC-157's gastroprotective properties may improve GI tolerability), GLP-1 therapy plus 5-Amino-1MQ for enhanced fat cell metabolism and NAD+ support, and GLP-1 therapy plus targeted exercise and nutritional programming designed to preserve lean mass during pharmacologically-driven weight loss. The peptide research hub and biohacking hub provide detailed coverage of these combination approaches and their evidence base.
Provider Selection and Quality of Care
The quality of GLP-1 therapy varies significantly based on prescriber expertise, monitoring protocols, and support services. Optimal GLP-1 care includes pre-treatment metabolic assessment (comprehensive metabolic panel, lipid panel, HbA1c, body composition analysis), individualized agent selection based on patient goals and characteristics, structured titration with regular tolerability assessment, ongoing monitoring of efficacy, side effects, and metabolic parameters, dietary and exercise counseling to maximize drug efficacy and preserve lean mass, and a long-term management plan that addresses treatment duration, dose optimization, and discontinuation strategy.
Patients should evaluate potential providers based on their experience with GLP-1 therapy (number of patients managed, familiarity with all available agents), their monitoring protocols (how frequently they check labs, body composition, and vital signs), their approach to side effect management (willingness to adjust dosing, switch agents, or add supportive therapies), their integration of lifestyle optimization (dietary counseling, exercise programming, behavioral support), and their availability for questions and concerns between scheduled visits. The dosing calculator and GLP-1 hub provide patient-facing resources that support informed conversations with providers and help patients evaluate the quality of care they're receiving.
Organ-Specific Outcomes: Liver, Kidney, and Metabolic Benefits Across the GLP-1 Class
While weight loss is the most visible outcome of GLP-1 therapy, the organ-specific benefits may ultimately prove more clinically significant for long-term health outcomes. GLP-1 agonists produce measurable improvements in liver fat content, kidney function markers, lipid profiles, and inflammatory biomarkers that extend far beyond what weight loss alone would predict. Understanding these organ-specific effects helps clinicians and patients appreciate the full therapeutic value of GLP-1 therapy.
Hepatic Benefits: NAFLD and NASH
Non-alcoholic fatty liver disease (NAFLD) affects approximately 30% of the global adult population and is the leading cause of chronic liver disease worldwide. Its progressive form, non-alcoholic steatohepatitis (NASH), involves hepatic inflammation and fibrosis that can progress to cirrhosis and hepatocellular carcinoma. GLP-1 agonists have emerged as the most promising pharmacological intervention for NAFLD/NASH, with effects that appear to extend beyond what weight loss alone would accomplish.
Semaglutide has the strongest hepatic data among GLP-1 agonists. In the Phase 2 NASH trial, semaglutide 0.4 mg daily produced NASH resolution (defined as disappearance of hepatic inflammation) in 59% of patients at 72 weeks, compared to 17% with placebo (p < 0.001). Hepatic fat content decreased by approximately 5-10 percentage points (absolute), and serum ALT (alanine aminotransferase) normalized in the majority of patients. The Phase 3 ESSENCE trial is evaluating semaglutide 2.4 mg weekly for histological improvement in NASH with fibrosis, with results expected in late 2026.
Tirzepatide's dual GLP-1/GIP mechanism may provide additional hepatic benefits through GIP-mediated effects on hepatic lipid metabolism. In the Combined effect-NASH trial (Phase 2), tirzepatide 15 mg produced NASH resolution in 74% of patients and fibrosis improvement in 47%, numbers that exceed semaglutide's Phase 2 results. However, cross-trial comparison is limited by different patient populations and study designs. Direct head-to-head data for hepatic outcomes are not yet available.
The mechanism of GLP-1-mediated liver benefit involves several pathways: reduced hepatic de novo lipogenesis (fatty acid synthesis in the liver), improved hepatic insulin sensitivity (reducing the insulin-driven fat accumulation that characterizes NAFLD), direct anti-inflammatory effects on hepatic Kupffer cells and stellate cells, and weight loss-mediated reduction in free fatty acid delivery to the liver from adipose tissue. The relative contribution of weight-dependent versus weight-independent mechanisms is still being determined, but studies showing liver fat reduction exceeding what would be predicted from weight loss alone suggest meaningful direct hepatic effects.
Renal Protection
The kidney is both a GLP-1 receptor-expressing organ and a major beneficiary of GLP-1-mediated metabolic improvements. The FLOW trial, the first dedicated kidney outcomes trial for a GLP-1 agonist, demonstrated that semaglutide 1.0 mg weekly reduced the risk of clinically significant kidney disease events by 24% (HR 0.76, 95% CI 0.66-0.88, p = 0.0003) in patients with type 2 diabetes and CKD. The kidney benefit was driven by reductions in persistent eGFR decline, end-stage kidney disease, and kidney-related death.
The mechanisms of renal protection include: reduction of glomerular hyperfiltration (a key driver of progressive kidney damage in diabetes), decreased albuminuria (reflecting improved glomerular barrier function), reduced renal inflammation, improved renal hemodynamics through natriuresis and blood pressure lowering, and weight loss-mediated reduction in the mechanical compression and metabolic stress that obesity places on kidney tissue.
For patients with CKD who are considering GLP-1 therapy, the agent selection matters. Semaglutide and tirzepatide are not primarily renally cleared and can be used without dose adjustment in CKD stages 1-4. Exenatide is renally cleared and should be avoided in patients with eGFR below 30 mL/min. Liraglutide and dulaglutide have intermediate renal clearance and can be used with caution in moderate CKD but have less strong kidney-specific outcome data than semaglutide.
Cardiovascular Biomarker Improvements
Beyond the MACE endpoint reductions demonstrated in cardiovascular outcome trials, GLP-1 agonists produce improvements across the full spectrum of cardiovascular risk biomarkers. In the SELECT trial, semaglutide 2.4 mg reduced C-reactive protein (CRP) by approximately 40% (indicating reduced systemic inflammation), reduced triglycerides by 15-25%, lowered systolic blood pressure by 3-5 mmHg, and improved heart rate variability (a marker of cardiac autonomic function). These biomarker improvements were partially but not entirely explained by weight loss, again suggesting direct cardiovascular effects of GLP-1 receptor activation.
The anti-inflammatory effects of GLP-1 agonists are particularly relevant because systemic inflammation is now recognized as a primary driver of atherosclerosis, plaque instability, and cardiovascular events. The CRP reduction with semaglutide (approximately 40%) approaches the magnitude seen with anti-inflammatory therapies specifically designed for cardiovascular protection (like canakinumab in the CANTOS trial, which reduced CRP by 40-60%). This inflammatory pathway may explain a significant portion of GLP-1 agonists' cardiovascular benefit, independent of weight loss and glucose control.
For patients and providers seeking to optimize cardiovascular protection with GLP-1 therapy, the GLP-1 research hub provides detailed analysis of cardiovascular outcome data across all agents, and the dosing calculator helps optimize dose selection for individual cardiovascular risk profiles. Complementary peptide approaches for cardiovascular support, including BPC-157 for vascular health and SS-31 for cardiac mitochondrial function, are covered in the peptide research hub.
GLP-1 Therapy in Special Populations: Tailoring Treatment to the Individual
One of the most common mistakes in GLP-1 prescribing is treating every patient the same way. A 65-year-old woman with type 2 diabetes, osteoporosis risk, and heart failure has profoundly different therapeutic needs than a 35-year-old male athlete looking to optimize body composition, or a 50-year-old prediabetic man with fatty liver disease. The clinical trial data give us population averages, but the art of GLP-1 therapy lies in adapting those averages to individual circumstances. This section covers what we know about GLP-1 response and safety across different patient groups.
Elderly Patients (Age 65+)
Older adults present a unique challenge with GLP-1 therapy because the goals and risks shift considerably compared to younger patients. The primary concern in this population is sarcopenia, the age-related loss of muscle mass that accelerates after age 60 and is independently associated with falls, fractures, disability, and mortality. GLP-1-induced weight loss in elderly patients produces lean mass losses of 25-40% of total weight lost, and when you're starting from an already depleted muscle reserve, this percentage translates to functionally meaningful weakness.
The STEP 2 subgroup analysis examined semaglutide 2.4 mg outcomes in patients aged 65 and older. Weight loss was slightly lower than in younger patients (approximately 12.5% vs. 15.3%), but the proportion of lean mass lost was higher (approximately 39% vs. 27% of total weight lost). This means that elderly patients may lose less fat relative to muscle, which is exactly the opposite of what clinicians want to achieve. Tirzepatide subgroup data from SURMOUNT-2 showed a similar pattern, with patients over 65 losing slightly less total weight but a higher fraction from lean tissue.
Practical modifications for elderly patients include slower dose titration (extending each dose step to 6-8 weeks instead of the standard 4), protein intake optimization (targeting 1.2-1.6 g/kg/day, considerably higher than typical elderly intake of 0.8-1.0 g/kg), concurrent resistance training (even light resistance exercise significantly reduces lean mass loss), and considering complementary peptides like CJC-1295/Ipamorelin that support lean tissue preservation through GH secretion. Bone density monitoring is also warranted, as rapid weight loss in elderly patients can accelerate bone mineral density decline independently of any direct GLP-1 effect on bone.
The cardiovascular benefits of GLP-1 therapy may be particularly valuable in elderly patients, who have the highest baseline cardiovascular risk. The SELECT trial showed that semaglutide reduced MACE events by 20% in patients with established cardiovascular disease, and subgroup analyses consistently showed equal or greater benefit in patients over 65. This creates a genuine clinical tension: the cardiovascular benefits of GLP-1 therapy in elderly patients are substantial, but the sarcopenia and frailty risks are also higher. Careful patient selection, aggressive lean mass preservation strategies, and regular functional assessments are essential. The dosing calculator can help providers identify appropriate starting doses and titration schedules for elderly patients.
Women: Hormonal Considerations and Reproductive Effects
GLP-1 therapy in women involves several sex-specific considerations that are underappreciated in clinical practice. First, women consistently show higher GI side effect rates than men across all GLP-1 agents, likely due to the interaction between GLP-1 signaling and estrogen-mediated effects on gastric motility. In the STEP trials, women had approximately 30% higher rates of nausea, vomiting, and constipation than men at the same doses, despite similar weight loss outcomes. This suggests that women may benefit from slower titration and more aggressive anti-nausea management.
Reproductive considerations are critically important and often inadequately addressed. GLP-1 receptor agonists can improve fertility in women with PCOS by improving insulin sensitivity, reducing androgen levels, and restoring ovulation. Several case reports and small studies have documented unexpected pregnancies in women who had previously been subfertile, occurring within the first 2-3 months of GLP-1 therapy. All GLP-1 agonists are classified as contraindicated in pregnancy due to animal reproductive toxicity data showing increased embryonic loss at supratherapeutic doses. Women of reproductive age must use reliable contraception, and GLP-1 therapy should be discontinued at least 2 months before planned conception (to allow for drug washout given the long half-lives of weekly agents).
Postmenopausal women face additional bone density concerns. Estrogen withdrawal already accelerates bone turnover, and the added metabolic stress of significant weight loss can compound this effect. Dual-energy X-ray absorptiometry (DXA) monitoring at baseline and after 6-12 months of treatment is reasonable in postmenopausal women on GLP-1 therapy, particularly those losing more than 10% body weight. Calcium and vitamin D supplementation should be optimized before starting therapy.
Body composition differences between men and women also affect response patterns. Women typically have higher body fat percentages and lower lean mass at any given BMI, which means that a 15% weight loss in a woman represents a different metabolic achievement than the same percentage in a man. Fat distribution also matters: women tend to lose preferentially from subcutaneous rather than visceral fat depots, while men show more balanced or visceral-predominant fat loss. Since visceral fat is more metabolically harmful, this difference may partially explain why men show slightly greater metabolic improvements (HbA1c reduction, lipid improvements, blood pressure reduction) at similar weight loss percentages.
Athletes and Active Individuals
The use of GLP-1 agonists in athletes and highly active individuals is a growing but controversial area. The clinical trial populations were largely sedentary, and extrapolating those results to people who train intensively introduces several unknowns. The primary concern is performance impairment from reduced caloric intake, delayed gastric emptying (which can cause nausea during exercise), and potential lean mass loss that directly impairs strength, power, and athletic capacity.
Athletes considering GLP-1 therapy for body composition optimization typically use lower doses than the maximum approved for obesity (for example, semaglutide 0.5-1.0 mg rather than 2.4 mg, or tirzepatide 5-7.5 mg rather than 15 mg). These lower doses provide meaningful fat loss while minimizing the appetite suppression that can prevent adequate fueling for training. Timing is also important: injecting GLP-1 medications 2-3 days before rest days or lower-intensity training sessions can minimize the impact of peak GI side effects on training quality.
The lean mass preservation concern is particularly acute in athletes, where every kilogram of muscle tissue contributes to performance. Combining GLP-1 therapy with adequate protein intake (2.0-2.4 g/kg for resistance-trained athletes), periodized resistance training, and potentially MK-677 or sermorelin for GH support can help maintain lean mass during fat loss phases. Some sports medicine providers also use BPC-157 concurrently to manage GI side effects and support recovery.
It's worth noting that WADA (World Anti-Doping Agency) does not currently list GLP-1 receptor agonists as prohibited substances, though this could change as athletic use becomes more prevalent. Athletes competing in sanctioned events should verify current prohibited lists before using any GLP-1 agent.
Patients with Type 1 Diabetes
GLP-1 therapy in type 1 diabetes is off-label but increasingly studied. The rationale includes reducing insulin requirements (GLP-1 agonists decrease glucagon secretion and slow gastric emptying, reducing postprandial glucose excursions), promoting weight loss (obesity affects 20-30% of type 1 diabetic adults), and potentially providing cardioprotective and renal-protective benefits independent of glucose control.
The ADJUNCT trials evaluated liraglutide as add-on therapy to insulin in type 1 diabetes. Results showed modest HbA1c reductions (0.2-0.4%), meaningful weight loss (approximately 5-7%), and reduced daily insulin requirements (approximately 10-15% reduction). However, there was a higher rate of hypoglycemia (particularly when insulin doses were not proactively reduced) and a signal for increased diabetic ketoacidosis (DKA) risk. The DKA concern relates to the dual insulin-reducing effects of GLP-1 therapy: less endogenous secretion plus patient/provider-initiated insulin dose reduction can sometimes create relative insulin deficiency in a patient who has no endogenous insulin production.
For type 1 diabetic patients on GLP-1 therapy, close monitoring of ketone levels, proactive (but cautious) insulin dose adjustment, and patient education about DKA warning signs are essential. This is a situation where specialized endocrine oversight is particularly valuable.
Patients with Chronic Kidney Disease
GLP-1 agonists have shown consistent renal protective effects across multiple trials, making CKD patients a particularly important population for these therapies. The FLOW trial demonstrated that semaglutide reduced the risk of clinically significant kidney events by 24% in patients with type 2 diabetes and CKD. This renal benefit appears to be partially independent of glucose and weight effects, suggesting direct protective mechanisms involving reduced glomerular hyperfiltration, decreased renal inflammation, and improved tubular function.
Dosing considerations vary by CKD stage. For stages 1-3a (eGFR > 45 mL/min), no dose adjustment is typically needed for any GLP-1 agonist. For stages 3b-4 (eGFR 15-44 mL/min), the available data support use of semaglutide, tirzepatide, and dulaglutide without dose adjustment, as these are not primarily renally cleared. Exenatide, which is renally cleared, should not be used in patients with eGFR below 30 mL/min. For stage 5 and dialysis patients, data are limited and GLP-1 therapy should be used with caution and close monitoring.
The GI side effects of GLP-1 therapy can interact with CKD management in important ways. Nausea, vomiting, and diarrhea can cause dehydration, which is poorly tolerated in CKD patients and can trigger acute kidney injury. Slower titration, aggressive hydration counseling, and close monitoring of renal function during the dose-escalation phase are standard practice in CKD patients. Providers working with CKD patients on GLP-1 therapy can use the GLP-1 research hub for detailed guidance on monitoring protocols and dose adjustment strategies.
Drug Interactions, Contraindications, and Perioperative Management
GLP-1 receptor agonists interact with other medications primarily through their effect on gastric emptying rather than through traditional cytochrome P450 enzyme interactions. This pharmacodynamic (rather than pharmacokinetic) interaction profile makes them generally well-tolerated in combination with most drugs, but there are several clinically significant exceptions and practical considerations that every patient and provider should understand.
Oral Medication Absorption Effects
By slowing gastric emptying, GLP-1 agonists delay the absorption of co-administered oral medications. For most drugs, this delay is clinically insignificant because total absorption (area under the curve) is preserved even though peak concentrations are reached later. However, for medications where absorption timing is critical, this delay can be problematic.
Oral contraceptives are the most commonly discussed interaction. GLP-1 agonists delay absorption of ethinyl estradiol and levonorgestrel by approximately 30-60 minutes, which reduces the peak concentration (Cmax) by 10-20% without meaningfully reducing total absorption. The clinical significance of this is debated, but given the consequences of contraceptive failure, most guidelines recommend using non-oral contraception (IUD, implant, patch) or adding barrier methods during GLP-1 therapy, especially during the dose-titration phase when gastric emptying effects are most variable.
Narrow therapeutic index drugs require more careful attention. Warfarin absorption can be delayed and more variable during GLP-1 therapy, and INR should be monitored more frequently during initiation and dose changes. Levothyroxine absorption is already highly sensitive to gastric pH and timing, and GLP-1-induced changes in gastric motility can alter thyroid hormone levels. Patients on levothyroxine should have TSH checked 6-8 weeks after starting GLP-1 therapy and after any dose changes. Anti-seizure medications (phenytoin, carbamazepine, valproic acid) should also be monitored more closely during GLP-1 initiation.
For patients taking oral semaglutide (Rybelsus), the timing requirements are particularly strict: the tablet must be taken on an empty stomach with no more than 4 oz of plain water, 30 minutes before any food, drink, or other medications. This is because oral semaglutide relies on a specific absorption enhancer (SNAC) that requires an acidic, fasted stomach environment to function. Taking other medications within the 30-minute window can dramatically reduce semaglutide absorption.
Diabetes Medication Interactions
When GLP-1 agonists are combined with other glucose-lowering medications, the risk of hypoglycemia varies by combination. Sulfonylureas (glipizide, glyburide, glimepiride) combined with GLP-1 agonists produce the highest hypoglycemia risk because both drug classes stimulate insulin secretion, but sulfonylureas do so in a glucose-independent manner. Current guidelines recommend reducing sulfonylurea doses by 50% when initiating GLP-1 therapy and monitoring blood glucose closely during titration.
Insulin and GLP-1 combinations are effective and widely used, but require proactive insulin dose reduction. The typical recommendation is to reduce basal insulin by 10-20% when starting a GLP-1 agonist and to reduce mealtime insulin by 20-30%, with further adjustments based on glucose monitoring. The FDA has approved fixed-ratio insulin/GLP-1 combinations (iDegLira: insulin degludec/liraglutide; iGlarLixi: insulin glargine/lixisenatide) that simplify this combination approach.
SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) combined with GLP-1 agonists represent a pharmacologically rational combination that provides complementary cardiovascular, renal, and metabolic benefits. The combination does not increase hypoglycemia risk (neither class causes glucose-independent insulin release) and produces additive weight loss. The main concern is additive dehydration from GI side effects (GLP-1) plus increased urinary glucose and fluid loss (SGLT2i), which requires attention to hydration status.
Absolute and Relative Contraindications
The absolute contraindications for GLP-1 receptor agonists include personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia type 2 (MEN2). This contraindication stems from preclinical findings in rodents showing thyroid C-cell tumors with chronic GLP-1 agonist exposure. While this effect has not been demonstrated in humans (human thyroid C-cells have fewer GLP-1 receptors than rodent C-cells), the contraindication remains in place as a precautionary measure. Calcitonin levels should be checked at baseline in patients with thyroid nodules or risk factors for MTC.
History of pancreatitis is a relative contraindication. GLP-1 agonists are not recommended in patients with active pancreatitis, and caution is advised in patients with a history of pancreatitis. However, the evidence linking GLP-1 therapy to pancreatitis causation is weak, and large cardiovascular outcome trials have not shown increased pancreatitis rates. The SUSTAIN and PIONEER trial programs for semaglutide showed pancreatitis rates of less than 0.5% in both treatment and placebo groups.
Pregnancy and breastfeeding are contraindications for all GLP-1 agonists based on animal reproductive toxicity data. Severe gastroparesis is a relative contraindication because GLP-1 agonists further slow gastric emptying, which can worsen symptoms and increase the risk of gastric bezoar formation. Patients with mild gastroparesis may tolerate GLP-1 therapy with careful monitoring, but those with severe or symptomatic gastroparesis should generally avoid these medications.
Perioperative Management
The American Society of Anesthesiologists (ASA) issued guidance in 2023 recommending that GLP-1 agonists be held before elective procedures requiring general anesthesia or procedural sedation. The concern is that GLP-1-induced delayed gastric emptying increases the risk of retained gastric contents and pulmonary aspiration during intubation or deep sedation.
Current ASA guidance recommends holding daily GLP-1 agonists (liraglutide, exenatide BID) for at least 24 hours before scheduled procedures, and holding weekly GLP-1 agonists (semaglutide, tirzepatide, dulaglutide) for at least one week before scheduled procedures. For urgent or emergent procedures where GLP-1 therapy has not been held, patients should be treated as having a full stomach regardless of fasting duration, with rapid sequence intubation and appropriate aspiration precautions.
Point-of-care gastric ultrasound is increasingly used to assess gastric volume in GLP-1 patients presenting for procedures. This bedside assessment can identify patients with significant retained gastric contents who would benefit from procedure delay, modified anesthesia technique, or pharmacological gastric emptying with prokinetic agents. Patients planning elective procedures should discuss GLP-1 medication timing with both their prescribing provider and their anesthesiologist.
Long-Term Outcomes, Treatment Durability, and the Weight Regain Question
The most pressing question in GLP-1 therapy today isn't which drug works best, but what happens when patients stop treatment and whether indefinite therapy is truly necessary. This question touches on the fundamental nature of obesity as a chronic disease, the durability of GLP-1-induced metabolic improvements, and the practical realities of lifelong injectable medication use.
Weight Regain After Discontinuation
The STEP 1 extension trial provided the most rigorous data on weight regain. After 68 weeks of semaglutide 2.4 mg therapy (producing approximately 17% weight loss), participants who switched to placebo regained approximately two-thirds of their lost weight over the following 52 weeks. The total weight from baseline at the end of the extension was approximately 5.6% below starting weight, compared to 17.3% at the end of active treatment. This means that substantial weight regain occurs, but patients don't fully return to baseline, at least within the observation period.
The SURMOUNT-4 trial for tirzepatide showed a remarkably similar pattern. After a 36-week open-label lead-in with tirzepatide (producing approximately 20% weight loss), patients randomized to placebo regained approximately 14% body weight over 52 weeks, while those continuing tirzepatide lost an additional 5.5%. The net difference between continuing versus stopping tirzepatide was approximately 19.5 percentage points at 88 weeks. These data strongly support the concept that GLP-1 therapy must be continued for sustained weight management, consistent with the chronic disease model of obesity.
However, the weight regain story has important nuances. Not all patients regain weight at the same rate. Approximately 15-20% of patients in extension studies maintained most of their weight loss after discontinuation, suggesting that some individuals achieve durable metabolic resetting that persists beyond drug treatment. Factors associated with sustained weight maintenance after GLP-1 discontinuation include greater physical activity level during treatment, higher dietary protein intake, resistance training participation, younger age, and shorter duration of obesity before treatment.
Metabolic Improvements: Do They Last?
Weight regain after GLP-1 discontinuation is accompanied by worsening of metabolic parameters, but the trajectory of metabolic deterioration doesn't perfectly mirror the weight trajectory. In the STEP 1 extension, HbA1c values worsened after semaglutide discontinuation but remained slightly improved from baseline even after one year off treatment. Blood pressure showed a similar pattern: partial regression toward baseline but not complete reversal. Lipid improvements (particularly triglyceride reductions) tended to reverse more completely, tracking closely with weight changes.
This dissociation between weight and metabolic outcomes suggests that GLP-1 therapy may produce some lasting metabolic benefits independent of weight maintenance. Possible mechanisms include sustained improvements in beta-cell function (GLP-1 agonists promote beta-cell survival and may partially reverse beta-cell dedifferentiation), persistent reductions in hepatic fat content (which doesn't fully reaccumulate at the same rate as subcutaneous fat), and behavioral changes (dietary preferences and eating patterns) that partially persist after drug discontinuation.
The cardiovascular outcome data add another dimension. The SELECT trial showed that semaglutide reduced MACE events in patients with established cardiovascular disease, with benefits becoming apparent after approximately 20 weeks and continuing to accrue throughout the 5-year trial. Whether these cardiovascular benefits persist after GLP-1 discontinuation is unknown, but the clinical experience with statins (where cardiovascular risk returns to baseline after discontinuation) suggests that continuous treatment may be needed for sustained cardiovascular protection.
Dose Reduction and Maintenance Strategies
An increasingly popular clinical approach is to use maximum doses during the active weight loss phase (typically 6-12 months) and then reduce to lower maintenance doses. The rationale is that lower doses may be sufficient to prevent weight regain once the initial weight loss has been achieved, while reducing side effect burden and medication costs. This approach has not been validated in large randomized trials, but emerging data from retrospective analyses and smaller studies are encouraging.
A retrospective analysis of patients who reduced semaglutide from 2.4 mg to 1.0 mg after achieving their weight loss goal showed that approximately 70% maintained within 5% of their lowest weight over 6-12 months on the lower dose. Those who regained significant weight on the lower dose could typically recapture their weight loss by returning to the full dose. Similar patterns have been observed with tirzepatide dose reductions, though the data are less mature.
Another maintenance strategy involves cycling: using GLP-1 therapy for defined periods (for example, 6 months on, 3 months off) rather than continuous treatment. The hypothesis is that periodic treatment can maintain most of the weight loss benefit while reducing total drug exposure, cost, and side effect burden. Early data suggest that cycling may work for some patients, particularly those who have established strong dietary and exercise habits during the "on" phases. However, other patients experience rapid weight regain during "off" phases that is psychologically discouraging and potentially metabolically harmful. Until more data are available, continuous therapy at the lowest effective dose remains the most evidence-supported maintenance strategy. The FormBlends assessment can help patients explore maintenance dosing options with their providers.
The Emerging Evidence for Combination Maintenance
Some clinicians are exploring whether non-GLP-1 therapies can partially substitute for GLP-1 agonists during the maintenance phase. The concept is to use GLP-1 therapy for initial weight loss, then transition to a less intensive (and less expensive) maintenance regimen that preserves most of the benefit. Candidates for maintenance combination therapy include AOD-9604 for continued fat metabolism support, 5-Amino-1MQ for NNMT inhibition and cellular fat metabolism, MOTS-c for mitochondrial metabolic optimization, and low-dose liraglutide (1.2-1.8 mg daily) as a less potent but less expensive GLP-1 option for maintenance.
These combination maintenance strategies are currently supported only by pharmacological rationale and limited clinical experience, not by randomized controlled trial data. Patients considering such approaches should do so under medical supervision with clear outcome tracking (weight, metabolic parameters, body composition) to assess effectiveness. The peptide research hub tracks emerging evidence for these combination protocols as new data become available.
Oral GLP-1 Agents and the Future of Drug Delivery
For many patients, the primary barrier to GLP-1 therapy isn't cost or side effects, but the requirement for self-injection. Needle phobia, injection fatigue, and the practical challenges of weekly injections (cold chain storage, travel with medications, disposal of sharps) limit adherence and discourage adoption. The pharmaceutical industry is aggressively pursuing oral, implantable, and other non-injectable delivery methods that could dramatically expand the GLP-1 patient population.
Oral Semaglutide: Lessons from Rybelsus
Rybelsus (oral semaglutide) was the first oral GLP-1 agonist approved for type 2 diabetes, reaching the market in 2019. It uses sodium N-[8-(2-hydroxybenzoyl)amino]caprylate (SNAC) as a permeation enhancer that transiently increases gastric pH and facilitates transcellular absorption of semaglutide across the gastric epithelium. The PIONEER trial program established its efficacy for diabetes management, with the highest approved dose of 14 mg daily producing HbA1c reductions of approximately 1.0-1.3%.
The limitations of Rybelsus illustrate the challenges of oral peptide delivery. The bioavailability of oral semaglutide is approximately 0.4-1.0%, meaning that 99% of each dose is destroyed in the GI tract. To deliver a pharmacologically effective amount, the oral dose (14 mg) must be approximately 50 times higher than the equivalent subcutaneous dose (0.25 mg). The strict fasting requirements (30 minutes before food, minimal water) further limit practical usability. And the lower achieved plasma levels compared to injectable semaglutide at therapeutic doses translate to less weight loss: oral semaglutide 14 mg produces approximately 4-5% weight loss, compared to 10-15% with injectable semaglutide 1.0-2.4 mg.
Higher-dose oral semaglutide (25 mg and 50 mg) is now being studied for obesity. The OASIS 1 trial showed that oral semaglutide 50 mg daily produced approximately 15.1% weight loss at 68 weeks, approaching the efficacy of injectable semaglutide 2.4 mg (which produced 14.9% in STEP 1). If approved, this higher-dose oral formulation would represent a meaningful option for patients who prefer pills over injections, though the fasting requirements and GI tolerability remain challenges.
Non-Peptide Oral GLP-1 Agonists
The most exciting development in GLP-1 delivery is the emergence of non-peptide, small molecule GLP-1 receptor agonists that can be taken orally without the absorption challenges of peptide drugs. These molecules are designed to bind and activate the GLP-1 receptor with high potency and selectivity while being orally bioavailable through conventional GI absorption mechanisms.
Orforglipron (Eli Lilly) is the most advanced non-peptide oral GLP-1 agonist. In the Phase 2 trial (GZGI study), orforglipron 45 mg daily produced approximately 14.7% weight loss at 36 weeks in patients with obesity. The Phase 3 ATTAIN trial program is currently enrolling, with results expected in 2026-2027. If successful, orforglipron would offer the first truly patient-friendly oral GLP-1 option: no fasting requirements, no injection needles, conventional storage, and easy travel compatibility.
Danuglipron (Pfizer) is another non-peptide oral GLP-1 agonist that showed promise in Phase 2 trials, with 12.7% weight loss at 32 weeks using the highest dose. However, high GI side effect rates (approximately 73% nausea) and the requirement for twice-daily dosing have raised questions about its competitive positioning. Pfizer has modified the formulation and dosing strategy, and Phase 3 trials are ongoing.
If non-peptide oral GLP-1 agonists achieve comparable efficacy to injectable agents (which the Phase 2 data suggest is possible), they could transform the obesity treatment landscape by removing the injection barrier. The potential market expansion is enormous: surveys consistently show that 30-40% of patients interested in GLP-1 therapy decline because of injection requirements. Making these therapies available as a daily pill could double or triple the treated population.
Long-Acting Implants and Monthly Formulations
On the other end of the convenience spectrum, several companies are developing long-acting GLP-1 delivery systems that would reduce dosing frequency from weekly to monthly or even less. Subcutaneous implants loaded with GLP-1 agonists could provide steady-state drug delivery for 3-6 months, eliminating the need for self-injection entirely while maintaining consistent plasma levels.
Monthly injectable formulations of semaglutide are also in development, using extended-release depot technologies that slowly release drug from a subcutaneous depot over 4 weeks. These formulations could reduce injection frequency by 75% while maintaining therapeutic drug levels, though they introduce a loss of dose flexibility (you can't easily adjust the dose once a depot injection has been administered).
These developments collectively point toward a future where GLP-1 therapy is available in multiple delivery formats tailored to individual patient preferences and clinical needs. Some patients will prefer the convenience and dose flexibility of weekly injections. Others will choose daily pills for their simplicity. Still others may opt for implants or monthly injections that minimize the cognitive burden of medication management. Compounding pharmacies like FormBlends are already exploring how these emerging delivery technologies can be integrated with existing peptide therapy protocols to maximize patient choice and adherence.
Global Access, Pricing Dynamics, and Health Equity Across the GLP-1 Class
The transformative clinical efficacy of GLP-1 receptor agonists has created one of the most significant access and affordability challenges in modern pharmaceutical history. With annual treatment costs ranging from $10,000 to $16,000 at list price in the United States, and global obesity affecting over 800 million people, the mathematics of universal access are staggering. Understanding the pricing dynamics, insurance coverage patterns, and emerging solutions for expanding access is essential for patients, providers, and policymakers alike.
Pricing Structures Across the Class
The wholesale acquisition cost (WAC) of branded GLP-1 agents in the U.S. varies considerably across the class. Semaglutide (Wegovy) carries a list price of approximately $1,350 per month, while tirzepatide (Zepbound) is priced at approximately $1,060 per month. Liraglutide (Saxenda) is priced at approximately $1,400 per month, despite producing substantially less weight loss than newer agents. These list prices rarely reflect what patients actually pay, as negotiated discounts, rebates, and patient assistance programs reduce the effective cost. However, the gap between list price and patient out-of-pocket cost varies enormously based on insurance coverage, formulary tier placement, and the specific terms of each plan.
International pricing comparisons reveal the scale of U.S. pricing premiums. Semaglutide for weight management costs approximately $300-400 per month in European markets, $150-200 per month in parts of Asia, and even less in countries that have negotiated volume-based pricing agreements with manufacturers. These price differences reflect the unique dynamics of the U.S. pharmaceutical market, including the lack of centralized price negotiation (though the Inflation Reduction Act is beginning to change this for Medicare), the role of pharmacy benefit managers in setting formulary terms, and the complex rebate structures that inflate list prices while reducing net prices through non-transparent channels.
Insurance Coverage Patterns
Insurance coverage for GLP-1 therapies prescribed for weight management varies dramatically by payer type and plan design. Among commercial insurers, coverage has expanded substantially since 2023, with approximately 40-50% of employer-sponsored plans now offering some form of coverage for anti-obesity medications. However, coverage is typically accompanied by significant restrictions: prior authorization requirements, BMI thresholds (usually requiring BMI of 30 or higher, or 27 with comorbidities), step therapy requirements (trying and failing cheaper alternatives first), and quantity limits.
Medicare, which covers approximately 66 million Americans, currently excludes anti-obesity medications from Part D coverage under a decades-old statutory exclusion. Legislative efforts to overturn this exclusion, including the Treat and Reduce Obesity Act, have gained bipartisan support but have not yet passed. The Congressional Budget Office estimates that Medicare coverage of GLP-1 agents for obesity would cost $35-50 billion over 10 years, a figure that has given legislators pause despite the potential for downstream savings in cardiovascular, diabetes, and joint-related healthcare costs.
Medicaid coverage varies by state, with some states covering anti-obesity medications and others excluding them. The patchwork nature of Medicaid coverage creates geographic disparities in access that disproportionately affect lower-income patients who bear the heaviest burden of obesity-related disease. States that have expanded Medicaid coverage for GLP-1 agents have generally seen lower rates of obesity-related hospitalizations, suggesting that medication access can reduce total healthcare costs even when the drug costs are substantial.
The Compounding Pharmacy Alternative
The shortage of branded semaglutide triggered an important development in GLP-1 access: the emergence of compounded semaglutide from FDA-registered 503A and 503B compounding pharmacies. Under FDA regulations, compounding pharmacies may produce patient-specific (503A) or batch (503B) preparations of drugs that are on the FDA's drug shortage list, provided they meet certain quality standards. Compounded semaglutide has dramatically expanded access for patients who cannot afford branded products or who face insurance barriers.
The cost differential is substantial. While branded Wegovy costs $1,300+ per month at list price, compounded semaglutide through services like FormBlends is available at a fraction of that cost, making GLP-1 therapy accessible to patients who would otherwise be priced out of treatment entirely. The quality and regulatory field of compounded peptides varies, however, and patients should seek compounding pharmacies that maintain strict quality controls, third-party testing, and transparent sourcing practices.
As the semaglutide shortage status evolves and branded manufacturers increase production capacity, the regulatory basis for compounding may shift. However, the fundamental access gap, between the number of patients who could benefit from GLP-1 therapy and the number who can afford branded products, is unlikely to close through manufacturing expansion alone. The role of compounding pharmacies in the GLP-1 access ecosystem will likely evolve rather than disappear, particularly as newer agents like CagriSema and retatrutide enter the market at premium price points.
Patient Assistance Programs and Savings Cards
Both Novo Nordisk and Eli Lilly offer manufacturer-sponsored savings programs that reduce out-of-pocket costs for commercially insured patients. These programs typically reduce copays to $25-150 per month for patients with qualifying insurance, though they do not apply to government-insured patients (Medicare, Medicaid, Tricare). The savings card programs have been instrumental in enabling initial access but create a sustainability concern: many patients who start therapy with a savings card face dramatic cost increases when the card expires or when coverage terms change.
Patient assistance programs (PAPs) for uninsured or underinsured patients exist but are less widely utilized. Income-based eligibility criteria, complex application processes, and limited supply allocations can make these programs difficult to access. Navigating the patchwork of assistance options requires either dedicated patient support staff or third-party navigation services, creating yet another barrier for patients in under-resourced settings.
Health Equity and Disparities in GLP-1 Access
The intersection of GLP-1 therapy access with existing health disparities deserves serious attention. Obesity prevalence is highest among Black, Hispanic, and American Indian/Alaska Native populations, yet these groups are significantly underrepresented among GLP-1 users. Multiple factors drive this disparity: lower rates of commercial insurance coverage, higher rates of Medicare and Medicaid enrollment (with their coverage limitations), fewer prescribers experienced in obesity pharmacotherapy in underserved communities, cultural and linguistic barriers to accessing weight management services, and historical medical mistrust that may reduce willingness to try injectable medications.
The research trial populations for most GLP-1 agents have also been disproportionately White, raising questions about whether efficacy and safety data are fully generalizable to diverse populations. While subgroup analyses generally suggest similar efficacy across racial and ethnic groups, sample sizes in these subgroups are often too small for definitive conclusions. Post-marketing studies with deliberate oversampling of underrepresented populations would strengthen the evidence base for equitable prescribing.
Addressing these disparities requires systemic interventions: policy changes to expand insurance coverage, investment in community-based obesity treatment programs, culturally adapted patient education materials, and deliberate efforts to ensure that cost-accessible options like compounded semaglutide reach the populations with the greatest unmet need. The GLP-1 research hub tracks evolving access and policy developments that affect patient access across the class.
International Perspectives and Global Health Impact
Outside the United States, GLP-1 access patterns reflect each country's healthcare system structure and pharmaceutical pricing policies. The United Kingdom's National Health Service (NHS) approved semaglutide for weight management in 2023, with specialist-led prescribing through designated weight management services. However, capacity constraints have limited uptake, with long waiting lists for weight management specialist appointments creating de facto rationing. Some UK patients have turned to private prescriptions or international pharmacies to access treatment more quickly.
In Nordic countries, where Novo Nordisk is headquartered, GLP-1 agents are broadly available but face periodic supply constraints. Japan, with a significant diabetes burden and growing obesity concern, has approved several GLP-1 agents for diabetes but has been slower to adopt weight-management indications. Australia's Pharmaceutical Benefits Scheme covers GLP-1 agents for diabetes but has faced budget pressure regarding weight management coverage expansion.
Perhaps the most significant global health question involves low- and middle-income countries (LMICs), where obesity rates are rising rapidly as urbanization and dietary shifts progress. Current GLP-1 pricing is entirely inaccessible for most LMIC healthcare systems and patients. The development of biosimilar GLP-1 agents, expected to begin entering the market as originator patents expire (semaglutide composition patents expire in the late 2020s to early 2030s depending on jurisdiction), could eventually broaden global access. However, biosimilar development for injectable peptides is technically complex and expensive, and significant price reductions may not materialize for several years after patent expiry. In the interim, public health strategies focused on dietary environment modification, physical activity promotion, and metabolic surgery capacity building remain the most feasible approaches for obesity management in resource-limited settings.
The Employer Health Plan Revolution
Some of the most significant developments in GLP-1 access are occurring at the employer level. Large self-insured employers, who directly bear the healthcare costs of their workforce, are increasingly adopting coverage of anti-obesity medications as a strategic investment in workforce health and productivity. Companies like Amazon, JPMorgan Chase, and Walmart have expanded coverage for GLP-1 agents, reasoning that the medication costs are partially offset by reduced claims for cardiovascular events, diabetes management, musculoskeletal procedures, and disability leave.
The employer perspective adds an economic dimension that pure clinical analyses miss. Obesity-related absenteeism and presenteeism (reduced productivity while present at work) cost U.S. employers an estimated $150-200 billion annually. If GLP-1 therapy can meaningfully reduce this burden, the business case for coverage becomes compelling even when drug costs are high. Early data from employer health plans that have covered GLP-1 agents for 2+ years show modest but real reductions in total healthcare spending for treated employees, though the results vary by industry and workforce demographics.
However, employer adoption creates its own equity concerns. Coverage decisions are made by benefits administrators and consultants who may apply criteria that inadvertently restrict access. Some employer plans cover GLP-1 agents for employees only, excluding dependents. Others impose step-therapy requirements that delay access or BMI thresholds that exclude patients who would still benefit from treatment. The variability in employer-plan design means that two workers at different companies with identical clinical profiles may face very different access to the same medication.
The Role of Telehealth in Democratizing Access
Telehealth platforms have emerged as a significant force in expanding GLP-1 access, particularly for patients in geographic areas with limited obesity medicine specialists. Direct-to-consumer telehealth services now offer online consultations, prescriptions for GLP-1 agents (including compounded formulations), and ongoing clinical monitoring through smartphone apps and remote vital sign tracking. This model bypasses many traditional barriers to access: no need for in-person specialist appointments, reduced wait times, and often more transparent pricing than traditional insurance-based models.
The quality of telehealth-based GLP-1 prescribing varies widely, however. At one end of the spectrum, well-designed platforms like FormBlends provide comprehensive clinical evaluation, structured follow-up protocols, and access to qualified prescribers experienced in metabolic medicine. At the other end, some services offer minimal clinical assessment, prescribe without adequate monitoring, and lack the infrastructure to manage complications or drug interactions. Patients evaluating telehealth options should look for platforms that require baseline lab work, provide ongoing monitoring guidance, offer access to clinical support for side effect management, and use licensed prescribers with training in obesity medicine or endocrinology.
The regulatory environment for telehealth prescribing of GLP-1 agents continues to evolve. The DEA's pandemic-era telehealth flexibilities have been extended, and many states have permanently expanded their telemedicine licensure requirements. However, specific regulations around prescribing injectable medications via telehealth, including requirements for in-person visits, prescriber-patient relationship establishment, and controlled substance rules (relevant for some compounds used alongside GLP-1 therapy), differ by state and are subject to change. Patients and providers should stay current with their state's telehealth regulations to ensure compliant prescribing practices.
Looking Forward: Pricing Pressures and the Generic Horizon
Several forces are converging to put downward pressure on GLP-1 pricing over the coming decade. The Inflation Reduction Act's drug price negotiation provisions will begin affecting Medicare Part D pricing for selected drugs, though GLP-1 agents for weight management are not currently eligible (due to the statutory exclusion of anti-obesity drugs from Part D coverage). If legislative changes extend Part D coverage to anti-obesity medications, these drugs could subsequently become subject to price negotiation, potentially reducing costs by 30-60% for Medicare beneficiaries.
Patent expirations represent the most certain source of future price relief. Liraglutide's key patents have begun expiring, and biosimilar development programs are underway. Semaglutide's composition patents face various expiration dates across jurisdictions through the late 2020s and into the 2030s, though formulation and process patents may extend exclusivity somewhat further. Tirzepatide, as a newer molecule, has patent protection extending into the 2030s. The development of biosimilar peptides is technically demanding and expensive, but the massive market size for GLP-1 agents has attracted significant investment from biosimilar developers worldwide.
The interplay between branded innovation, compounding pharmacy access, and eventual biosimilar competition will shape the GLP-1 pricing landscape for years to come. For patients seeking treatment today, the most practical approach is working with providers who can help access the most cost-effective option, whether that's branded medication through insurance, savings card programs, compounded formulations through qualified pharmacies, or clinical trial participation for next-generation agents. The GLP-1 research hub maintains current information on pricing, access programs, and emerging options across the class.
Ultimately, the story of GLP-1 access is one of extraordinary medical progress running headlong into economic reality. The clinical evidence supporting these medications is among the strongest in all of metabolic medicine. The weight loss efficacy exceeds anything previously achievable with pharmacotherapy alone. The cardiovascular benefits are proven in large randomized trials. And yet, the majority of people who could benefit from GLP-1 therapy worldwide currently cannot access it, due to cost, insurance barriers, geographic limitations, or simple lack of awareness. Closing this gap is one of the defining public health challenges of the current decade, and progress will require coordinated efforts from manufacturers, payers, policymakers, healthcare systems, and patient advocacy organizations. For individuals seeking access today, understanding the full range of options, from branded products and insurance pathways to compounded formulations and patient assistance programs, empowers informed decision-making in a complex and rapidly evolving marketplace.
Monitoring, Lab Work, and Clinical Follow-Up During GLP-1 Therapy
Effective GLP-1 therapy requires more than simply prescribing a medication and checking weight at follow-up visits. A structured monitoring protocol ensures that metabolic benefits are being realized, potential adverse effects are detected early, and treatment is adjusted based on objective data rather than subjective impressions alone. While no universally standardized monitoring protocol exists for GLP-1 therapy, clinical practice guidelines and expert consensus offer a reasonable framework that applies across the class.
Baseline Assessments Before Starting Treatment
Before initiating any GLP-1 receptor agonist, a comprehensive baseline assessment serves multiple purposes: it identifies contraindications, establishes reference values for monitoring therapeutic response, and documents the patient's metabolic status for insurance authorization purposes. The recommended baseline workup includes a complete metabolic panel (CMP), HbA1c (regardless of diabetes status, as it establishes glycemic baseline), fasting lipid panel, liver function tests (ALT, AST, GGT), thyroid function (TSH, and calcitonin if family history of medullary thyroid carcinoma), fasting insulin with calculated HOMA-IR, complete blood count, and vitamin D level.
Body composition assessment at baseline provides valuable context beyond simple weight measurement. Dual-energy X-ray absorptiometry (DEXA) scanning quantifies fat mass, lean mass, and bone mineral density, creating reference points for monitoring body composition changes throughout treatment. While DEXA is not universally available or insurance-covered for this indication, it provides the most accurate assessment of whether weight loss is coming predominantly from fat (desirable) or includes excessive lean mass loss (concerning). For patients who cannot access DEXA, bioelectrical impedance analysis (BIA) devices, while less accurate on an absolute basis, provide reasonable trending data when measured consistently on the same device.
Waist circumference measurement is a simple, free, and clinically meaningful metric that correlates with visceral adipose tissue and cardiometabolic risk. Changes in waist circumference often track more closely with metabolic improvement than changes in body weight, particularly in patients who are simultaneously gaining lean mass through exercise. Recording waist circumference at baseline and at each follow-up visit takes minimal time and adds genuine clinical value.
Monitoring During Dose Escalation (Weeks 0-16)
The dose-escalation phase is the period of highest GI side effect risk and requires the most attentive monitoring. Clinical visits or telehealth check-ins every 2-4 weeks during escalation allow providers to assess tolerability, adjust escalation timing, and address concerns before they lead to discontinuation. Key monitoring points during this phase include weight measurement, blood pressure assessment, symptom review (focusing on nausea, vomiting, constipation, diarrhea, and abdominal pain), dietary intake assessment (ensuring adequate protein and micronutrient consumption despite reduced appetite), and hydration status evaluation.
For patients taking semaglutide or tirzepatide, the standard escalation protocols can be modified based on individual tolerability. Patients experiencing significant GI symptoms may benefit from extending each dose step by 2-4 additional weeks before escalating further. Conversely, patients tolerating escalation well may proceed on the standard schedule or, in some cases, escalate slightly faster under close supervision. The FormBlends dosing calculator can assist with individualized escalation planning based on tolerability and response patterns.
Blood glucose monitoring deserves particular attention during escalation for patients with type 2 diabetes, especially those taking sulfonylureas or insulin. The glucose-lowering effects of GLP-1 agents can cause hypoglycemia when combined with these medications, requiring proactive dose reductions of the sulfonylurea or insulin as the GLP-1 dose increases. A reasonable approach is to reduce sulfonylurea doses by 50% at GLP-1 initiation and further adjust based on glucose monitoring data. Insulin-treated patients may need more granular dose adjustments guided by frequent self-monitoring or continuous glucose monitoring data.
Maintenance Phase Monitoring (After Reaching Target Dose)
Once patients reach their maintenance dose and GI side effects have stabilized, monitoring frequency can be reduced to every 3-6 months for most patients. Each maintenance visit should include weight measurement, blood pressure, and a focused clinical assessment. Laboratory monitoring at the 3-month, 6-month, and 12-month marks should include HbA1c, fasting lipid panel, liver function tests, and renal function. These tests track the metabolic benefits of therapy and provide early detection of any concerning trends.
Annual assessments should be more comprehensive, adding thyroid function testing, vitamin B12 level (as GLP-1 agonists may reduce B12 absorption through altered gastric acid secretion), vitamin D level, iron studies, and body composition assessment (DEXA or BIA). For patients who have lost more than 15% of body weight, annual DEXA scanning for bone density monitoring is particularly relevant, as significant weight loss can affect bone mineral density. Patients showing declining bone density may benefit from supplemental calcium and vitamin D, weight-bearing exercise prescription, or consultation with an endocrinologist for further evaluation.
Nutritional Monitoring and Deficiency Prevention
The profound appetite suppression achieved with GLP-1 agents, particularly the more potent agents like tirzepatide and combination therapies, creates genuine risk of nutritional inadequacy. When patients reduce their caloric intake by 30-50%, as is common with these medications, micronutrient intake can fall below recommended levels even with reasonably balanced food choices. Protein intake is the most critical nutritional parameter to monitor, as inadequate protein accelerates lean mass loss and compromises immune function, wound healing, and hair health.
A practical protein target for patients on GLP-1 therapy is 1.2-1.6 grams per kilogram of ideal body weight daily, consumed across 3-4 meals. For a patient with an ideal body weight of 75 kg, this translates to approximately 90-120 grams of protein daily. Many patients on GLP-1 therapy report consuming fewer than 60 grams daily unless specifically counseled on protein prioritization. Protein-forward meal planning, where protein is selected first and other macronutrients fill the remaining caloric budget, helps ensure adequacy without requiring patients to eat beyond their appetite.
Common micronutrient deficiencies to monitor include iron (especially in premenopausal women), vitamin B12, folate, vitamin D, calcium, magnesium, and zinc. A daily multivitamin with minerals provides reasonable baseline coverage, but patients with identified deficiencies may require targeted supplementation at higher doses. Patients who experience persistent vomiting or very low food intake may be at particular risk for thiamine deficiency, which can cause serious neurological complications if unrecognized. Providers should maintain awareness of this possibility, especially in patients who lose weight very rapidly.
Hair loss is one of the most commonly reported cosmetic concerns among patients on GLP-1 therapy, occurring in approximately 3-6% of patients across trials. While typically classified as telogen effluvium (a temporary shedding pattern triggered by metabolic stress), it can be distressing for patients and occasionally leads to therapy discontinuation. Ensuring adequate protein, iron, zinc, and biotin intake can help mitigate hair thinning. Patients who experience persistent hair loss beyond 6 months may benefit from dermatological evaluation to rule out other contributing factors. Reassuringly, telogen effluvium is typically self-limiting and resolves within 6-12 months even with continued therapy, as the body adapts to its new metabolic state.
Gastrointestinal nutrient absorption may also be affected by the altered gut motility induced by GLP-1 therapy. Slowed gastric emptying changes the timing and potentially the efficiency of nutrient absorption, particularly for minerals that are absorbed in specific segments of the GI tract under conditions of controlled pH and transit time. While clinically significant malabsorption is uncommon with GLP-1 agents at standard doses, patients who experience persistent diarrhea or very rapid weight loss should have nutritional status assessed comprehensively, including fat-soluble vitamins (A, D, E, K) and essential minerals. Complementary peptide therapies like BPC-157 have been studied in preclinical models for their effects on gastrointestinal mucosal health, though human data remain limited.
Psychological and Behavioral Monitoring
The psychological dimensions of GLP-1 therapy deserve as much monitoring attention as the metabolic parameters. Screening for depression and anxiety using validated instruments (such as the PHQ-9 and GAD-7) at baseline and at regular intervals helps identify patients who may need additional psychological support. Changes in eating behavior should be assessed qualitatively, with attention to both positive changes (reduced binge eating, less food preoccupation) and concerning patterns (food avoidance, excessive restriction, development of disordered eating attitudes).
Body image adjustment is another important psychological domain that clinicians should address. Rapid weight loss can create a dissonance between a patient's internal self-image and their changing physical appearance. Some patients report feeling like they don't recognize themselves or feeling uncomfortable in social situations despite losing weight they had wanted to lose. Others develop concerns about loose skin, facial volume loss, or the cosmetic effects of rapid weight change. Normalizing these experiences and connecting patients with appropriate psychological resources when needed supports overall treatment success. Complementary approaches to skin health and appearance concerns may include peptides like GHK-Cu, which has been studied for its skin-rejuvenating properties, though patients should discuss all supplementary approaches with their healthcare provider.
When to Consider Dose Adjustment or Discontinuation
Several clinical scenarios warrant reconsideration of the current GLP-1 regimen. Weight loss plateau, defined as less than 1% body weight change over 12 weeks at the maximum tolerated dose, may indicate the need for adjunctive therapy, lifestyle intervention intensification, or switching to a different agent. Persistent severe GI symptoms despite adequate dose escalation time (more than 8 weeks at maintenance dose) may require dose reduction or switching to a different agent with a distinct receptor binding profile.
New-onset pancreatitis symptoms (severe epigastric pain radiating to the back), acute gallbladder disease, or unexplained elevations in lipase or amylase should prompt immediate therapy discontinuation pending clinical evaluation. Pregnancy or planned pregnancy requires discontinuation with appropriate washout periods based on the specific agent's half-life. Significant weight loss beyond the patient's target, particularly if accompanied by sarcopenia or malnutrition, may warrant dose reduction to slow the rate of weight loss while maintaining metabolic benefits.
The monitoring framework described here represents best practice but should be adapted to individual patient circumstances, healthcare system resources, and provider capacity. Even a simplified version of this monitoring approach, including regular weight checks, basic metabolic labs, and dietary assessments, substantially improves outcomes compared to the common practice of prescribing a GLP-1 agent with minimal follow-up. Patients working with FormBlends receive structured monitoring guidance as part of their treatment protocol, ensuring that therapy is supported by appropriate clinical oversight throughout the treatment journey.
For patients using GLP-1 therapy in combination with other peptide protocols, such as growth hormone secretagogues like CJC-1295/Ipamorelin or metabolic peptides like MOTS-c, the monitoring framework should be expanded to include IGF-1 levels, fasting glucose trends, and any parameters specific to the additional compounds. The interaction between GLP-1 therapy and other peptide protocols has not been systematically studied in clinical trials, making careful clinical monitoring even more important when multiple agents are used concurrently. Providers experienced in peptide therapy can help design integrated monitoring protocols that account for the unique pharmacological interactions between these compounds. Regular communication between all treating providers ensures that monitoring data is shared and clinical decisions are coordinated across the patient's entire therapeutic regimen.
Frequently Asked Questions
1. What are GLP-1 receptor agonists and how do they work?
GLP-1 receptor agonists are a class of medications that mimic the action of glucagon-like peptide-1, a hormone naturally produced in your gut after eating. They work by binding to GLP-1 receptors in the pancreas (stimulating insulin and suppressing glucagon), the brain (reducing appetite and increasing satiety), and the stomach (slowing gastric emptying). The net effect is lower blood sugar, reduced food intake, and weight loss. Different agents in the class target additional receptors - tirzepatide also activates GIP receptors, while retatrutide activates GLP-1, GIP, and glucagon receptors simultaneously.
2. Which GLP-1 drug produces the most weight loss?
Among approved medications, tirzepatide (Zepbound) at 15 mg weekly produces the most weight loss - approximately 20.9% of body weight over 72 weeks in the SURMOUNT-1 trial. Semaglutide 2.4 mg (Wegovy) is second at approximately 14.9%. In clinical development, retatrutide has shown 24.2% weight loss in Phase 2 trials. Keep in mind that real-world results are typically 30-50% lower than clinical trial figures due to differences in adherence and lifestyle support.
3. How do the different GLP-1 drugs compare for type 2 diabetes?
For glucose control measured by HbA1c reduction, tirzepatide 15 mg leads the class with reductions of 2.1-2.4%, followed by semaglutide 1.0 mg at 1.5-1.8%, dulaglutide 1.5 mg at 1.1-1.5%, and liraglutide 1.8 mg at 1.0-1.5%. In the SURPASS-2 head-to-head trial, all three tirzepatide doses produced greater HbA1c reduction than semaglutide 1.0 mg. Tirzepatide also achieved the highest rates of patients reaching normal HbA1c levels below 5.7%, with 51% of patients achieving this threshold in SURPASS-2.
4. What is the difference between GLP-1 and GIP?
GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide) are both incretin hormones released from the gut after meals, but they differ in important ways. GLP-1 is secreted by L-cells in the lower intestine and powerfully suppresses appetite through brain receptors. GIP is secreted by K-cells in the upper intestine and has traditionally been viewed as primarily an insulin-stimulating hormone. When combined as agonists in tirzepatide, GIP appears to potentiate GLP-1's weight loss effects through complementary brain circuits while also improving beta cell function through additive signaling pathways.
5. Are all GLP-1 drugs essentially the same?
No. While they share a common mechanism of GLP-1 receptor activation, the drugs differ substantially in molecular structure, half-life, receptor selectivity, dosing frequency, efficacy, and side effect profiles. Exenatide is based on a lizard peptide and requires twice-daily dosing. Semaglutide is a modified human GLP-1 with a 7-day half-life. Tirzepatide is a dual GIP/GLP-1 agonist with a different receptor profile entirely. These structural differences translate to clinically meaningful differences in weight loss (ranging from 3% to 21%), glycemic control, and tolerability.
6. Which GLP-1 agonist has the fewest side effects?
Dulaglutide (Trulicity) consistently shows the lowest rates of GI side effects across clinical trials, with nausea rates of 12-15% compared to 20-44% for other agents. Tirzepatide has a better side effect profile than you'd expect given its superior efficacy - nausea rates of 18-26% at the 5-15 mg doses, lower than semaglutide 2.4 mg despite producing more weight loss. If tolerability is the top priority and maximum weight loss is less critical, dulaglutide offers the gentlest introduction to the GLP-1 class.
7. What is the cheapest GLP-1 medication?
At US list prices, exenatide (Byetta/Bydureon) is the least expensive at approximately $800-900 per month, but it's also the least effective for weight loss. Among more commonly prescribed agents, dulaglutide and semaglutide (Ozempic) are in the $950-1,000/month range. With insurance, copays can be as low as $25/month with manufacturer savings cards. For patients without insurance, compounded formulations of semaglutide and tirzepatide through providers like FormBlends typically cost $200-500/month.
8. Can you switch between different GLP-1 drugs?
Yes, switching between GLP-1 agonists is common and safe. When switching between once-weekly agents, start the new drug on the day the next dose of the old drug would be due. Begin at the lowest dose and follow the standard titration schedule. GI tolerance built on one agent doesn't fully transfer to another, so expect some return of nausea during the adjustment period. No washout period is needed between agents. Common reasons for switching include inadequate weight loss, persistent side effects, insurance coverage changes, or upgrading to a newer agent like tirzepatide.
9. Do GLP-1 drugs protect the heart?
Several do, yes. Liraglutide (LEADER trial), semaglutide (SUSTAIN-6 and SELECT trials), and dulaglutide (REWIND trial) have all demonstrated statistically significant reductions in major adverse cardiovascular events (MACE) - typically 12-20% lower risk. Semaglutide has the broadest evidence, including SELECT, which showed 20% MACE reduction in patients with obesity but without diabetes. Exenatide showed non-inferiority but not superiority for CV outcomes. Tirzepatide's cardiovascular outcomes trial is still ongoing.
10. What happens when you stop taking a GLP-1 agonist?
Weight regain is the primary concern. In the STEP 1 extension study, patients who discontinued semaglutide 2.4 mg regained approximately two-thirds of their lost weight within one year. Blood sugar levels also return toward pre-treatment values in patients with diabetes. This is consistent with GLP-1 agonists treating the underlying biological drivers of obesity (appetite dysregulation) rather than curing them. Most guidelines now recommend treating GLP-1 agonists as chronic therapy, similar to blood pressure or cholesterol medications.
11. Is there an oral GLP-1 drug available?
Oral semaglutide (Rybelsus) is currently the only approved oral GLP-1 receptor agonist. It must be taken daily on an empty stomach with minimal water, and its bioavailability is only about 1%. A new oral small-molecule GLP-1 agonist called orforglipron is in Phase 3 trials and doesn't require fasting restrictions. Another oral compound, amycretin (an amylin/GLP-1 dual agonist), showed 13% weight loss at just 12 weeks in Phase 2. Oral GLP-1 options are expected to expand significantly by 2027-2028.
12. What is the difference between Ozempic, Wegovy, Mounjaro, and Zepbound?
Ozempic and Wegovy are both semaglutide but at different doses for different indications. Ozempic (0.25-2.0 mg) is approved for type 2 diabetes; Wegovy (2.4 mg) is approved for obesity. Mounjaro and Zepbound are both tirzepatide - Mounjaro for diabetes, Zepbound for obesity. The key clinical difference is that tirzepatide (Mounjaro/Zepbound) is a dual GIP/GLP-1 agonist that produces more weight loss and glycemic improvement than semaglutide (Ozempic/Wegovy), which is a pure GLP-1 agonist.
13. Can GLP-1 drugs cause thyroid cancer?
In rodent studies, GLP-1 agonists caused thyroid C-cell tumors (medullary thyroid carcinoma). However, this appears to be rodent-specific. Human thyroid C-cells express far fewer GLP-1 receptors than rodent C-cells. Over 15 years of human clinical trial data and post-marketing surveillance have not shown an increased risk of thyroid cancer. Despite this reassuring human data, all GLP-1 agonists carry a boxed warning and are contraindicated in patients with a personal or family history of medullary thyroid carcinoma or MEN2 syndrome.
14. How do I choose between semaglutide and tirzepatide?
The choice depends on your primary treatment goal, tolerance for side effects, insurance coverage, and whether you have diabetes. If maximum weight loss is the goal, tirzepatide is superior (20.9% vs. 14.9% in obesity trials). If proven cardiovascular protection matters most, semaglutide currently has stronger evidence (SELECT trial). Tirzepatide tends to have a more favorable GI side effect profile relative to its efficacy. Insurance formulary placement often makes the final decision - check with your plan to see which is covered at a lower tier.
15. What new GLP-1 drugs are coming in the next few years?
The pipeline is extensive. Retatrutide (Eli Lilly's triple GLP-1/GIP/glucagon agonist) showed 24.2% weight loss in Phase 2 and is in Phase 3 trials. Orforglipron (Eli Lilly) is an oral non-peptide GLP-1 agonist that doesn't require fasting. CagriSema (Novo Nordisk) combines amylin and semaglutide and showed 22.7% weight loss. Survodutide (Boehringer Ingelheim) targets GLP-1/glucagon for both obesity and fatty liver disease. Several of these could receive approval in 2027-2028, offering patients even more effective options than currently available.
References
- Eng J. Exendin peptides. Mt Sinai J Med. 1992;59(2):147-149.
- DeFronzo RA, Ratner RE, Han J, et al. Effects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetes. Diabetes Care. 2005;28(5):1092-1100. DOI: 10.2337/diacare.28.5.1092
- Buse JB, Henry RR, Han J, et al. Effects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetes. Diabetes Care. 2004;27(11):2628-2635. DOI: 10.2337/diacare.27.11.2628
- Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet. 2006;368(9548):1696-1705. DOI: 10.1016/S0140-6736(06)69705-5
- Holst JJ. The physiology of glucagon-like peptide 1. Physiol Rev. 2007;87(4):1409-1439. DOI: 10.1152/physrev.00034.2006
- Garber AJ, King AB, Del Prato S, et al. Insulin degludec, an ultra-longacting basal insulin, versus insulin glargine in basal-bolus treatment with mealtime insulin aspart in type 2 diabetes (BEGIN Basal-Bolus Type 2). Lancet. 2012;379(9825):1498-1507.
- Marre M, Shaw J, Brandle M, et al. Liraglutide, a once-daily human GLP-1 analogue, added to a sulphonylurea over 26 weeks produces greater improvements in glycaemic and weight control compared with adding rosiglitazone or placebo in subjects with type 2 diabetes (LEAD-1 SU). Diabet Med. 2009;26(3):268-278. DOI: 10.1111/j.1464-5491.2009.02666.x
- Marso SP, Daniels GH, Tanaka-Kido K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311-322. DOI: 10.1056/NEJMoa1603827
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844. DOI: 10.1056/NEJMoa1607141
- Holman RR, Bethel MA, Mentz RJ, et al. Effects of once-weekly exenatide on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2017;377(13):1228-1239. DOI: 10.1056/NEJMoa1612917
- Hernandez AF, Green JB, Janmohamed S, et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes). Lancet. 2018;392(10157):1519-1529. DOI: 10.1016/S0140-6736(18)32261-X
- Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND). Lancet. 2019;394(10193):121-130. DOI: 10.1016/S0140-6736(19)31149-3
- Husain M, Birkenfeld AL, Donsmark M, et al. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2019;381(9):841-851. DOI: 10.1056/NEJMoa1901118
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221-2232. DOI: 10.1056/NEJMoa2307563
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183
- Davies M, Faerch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2). Lancet. 2021;397(10278):971-984. DOI: 10.1016/S0140-6736(21)00213-0
- Wadden TA, Bailey TS, Billings LK, et al. Effect of subcutaneous semaglutide vs placebo as an adjunct to intensive behavioral therapy on body weight in adults with overweight or obesity (STEP 3). JAMA. 2021;325(14):1403-1413. DOI: 10.1001/jama.2021.1831
- Rubino D, Abrahamsson N, Davies M, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity (STEP 4). JAMA. 2021;325(14):1414-1425. DOI: 10.1001/jama.2021.3224
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(4):327-340. DOI: 10.1056/NEJMoa2206038
- Garvey WT, Frias JP, Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes (SURMOUNT-2). Lancet. 2023;402(10402):613-626. DOI: 10.1016/S0140-6736(23)01200-X
- Frias JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med. 2021;385(6):503-515. DOI: 10.1056/NEJMoa2107519
- Del Prato S, Kahn SE, Pavo I, et al. Tirzepatide versus insulin glargine in type 2 diabetes and increased cardiovascular risk (SURPASS-4). Lancet. 2021;398(10313):1811-1824. DOI: 10.1016/S0140-6736(21)02188-7
- Rosenstock J, Wysham C, Frias JP, et al. Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1). Lancet. 2021;398(10295):143-155. DOI: 10.1016/S0140-6736(21)01324-6
- Jastreboff AM, Kaplan LM, Frias JP, et al. Triple-hormone-receptor agonist retatrutide for obesity. N Engl J Med. 2023;389(6):514-526. DOI: 10.1056/NEJMoa2301972
- Aronne LJ, Sattar N, Horn DB, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity (SURMOUNT-4). JAMA. 2024;331(1):38-48. DOI: 10.1001/jama.2023.24945
- Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management (SCALE Obesity and Prediabetes). N Engl J Med. 2015;373(1):11-22. DOI: 10.1056/NEJMoa1411892
- Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. 2021;46:101102. DOI: 10.1016/j.molmet.2020.101102
- Knop FK, Aroda VR, do Vale RD, et al. Oral semaglutide 50 mg taken once daily in adults with overweight or obesity (OASIS 1). Lancet. 2023;402(10403):705-719. DOI: 10.1016/S0140-6736(23)01185-6
- Frias JP, Hsia S, Eyde S, et al. Efficacy and safety of oral orforglipron in patients with type 2 diabetes. N Engl J Med. 2023;389(10):877-888. DOI: 10.1056/NEJMoa2303601
- Wharton S, Blevins T, Connery L, et al. Daily oral GLP-1 receptor agonist orforglipron for adults with obesity. N Engl J Med. 2023;389(10):877-888. DOI: 10.1056/NEJMoa2302392
- Newsome PN, Buchholtz K, Cusi K, et al. A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. N Engl J Med. 2021;384(12):1113-1124. DOI: 10.1056/NEJMoa2028395
- Sanyal AJ, Bedossa P, Engell L, et al. A phase 2 randomized trial of survodutide in MASH and fibrosis. N Engl J Med. 2024;391(4):311-319. DOI: 10.1056/NEJMoa2401755
- Pratley RE, Aroda VR, Lingvay I, et al. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7). Lancet Diabetes Endocrinol. 2018;6(4):275-286. DOI: 10.1016/S2213-8587(18)30024-X
- Capehorn MS, Catarig AM, Furberg JK, et al. Efficacy and safety of once-weekly semaglutide 1.0 mg vs once-daily liraglutide 1.2 mg as add-on to 1-3 oral antidiabetic medications in subjects with type 2 diabetes (SUSTAIN 10). Diabetes Metab. 2020;46(2):100-109. DOI: 10.1016/j.diabet.2019.101117
- Dungan KM, Povedano ST, Forst T, et al. Once-weekly dulaglutide versus once-daily liraglutide in metformin-treated patients with type 2 diabetes (AWARD-6). Lancet. 2014;384(9951):1349-1357. DOI: 10.1016/S0140-6736(14)60976-4
- Gerstein HC, Sattar N, Rosenstock J, et al. Cardiovascular and renal outcomes with efpeglenatide in type 2 diabetes. N Engl J Med. 2021;385(10):896-907. DOI: 10.1056/NEJMoa2108269
- Perkovic V, Tuttle KR, Rossing P, et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N Engl J Med. 2024;391(2):109-121. DOI: 10.1056/NEJMoa2403347
- Kosiborod MN, Abildstrom SZ, Borlaug BA, et al. Semaglutide in patients with heart failure with preserved ejection fraction and obesity. N Engl J Med. 2023;389(12):1069-1084. DOI: 10.1056/NEJMoa2306963
- Sattar N, McGuire DK, Pavo I, et al. Tirzepatide cardiovascular event risk assessment: a pre-specified meta-analysis. Nat Med. 2022;28(3):591-598. DOI: 10.1038/s41591-022-01707-4
- Rubino DM, Greenway FL, Khalid U, et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body weight in adults with overweight or obesity without diabetes (STEP 8). JAMA. 2022;327(2):138-150. DOI: 10.1001/jama.2021.23619
- Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide (STEP 1 extension). Diabetes Obes Metab. 2022;24(8):1553-1564. DOI: 10.1111/dom.14725
- Drucker DJ. The GLP-1 journey: from discovery science to therapeutic impact. J Clin Invest. 2024;134(2):e175634. DOI: 10.1172/JCI175634
- Campbell JE, Drucker DJ. Pharmacology, physiology, and mechanisms of incretin hormone action. Cell Metab. 2013;17(6):819-837. DOI: 10.1016/j.cmet.2013.04.008
- Muller TD, Finan B, Bloom SR, et al. Glucagon-like peptide 1 (GLP-1). Mol Metab. 2019;30:72-130. DOI: 10.1016/j.molmet.2019.09.010
- Nauck MA, Meier JJ. GIP and GLP-1: stepsiblings rather than monozygotic twins within the incretin family. Diabetes. 2019;68(5):897-900. DOI: 10.2337/dbi19-0005
- Samms RJ, Coghlan MP, Sloop KW. How may GIP enhance the therapeutic efficacy of GLP-1? Trends Endocrinol Metab. 2020;31(6):410-421. DOI: 10.1016/j.tem.2020.02.006
- Day JW, Ottaway N, Patterson JT, et al. A new glucagon and GLP-1 co-agonist eliminates obesity in rodents. Nat Chem Biol. 2009;5(10):749-757. DOI: 10.1038/nchembio.209
- Finan B, Yang B, Ottaway N, et al. A rationally designed monomeric peptide triagonist corrects obesity and diabetes in rodents. Nat Med. 2015;21(1):27-36. DOI: 10.1038/nm.3761
- Rosenstock J, Frias J, Jastreboff AM, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes. Lancet. 2023;402(10401):529-544. DOI: 10.1016/S0140-6736(23)01053-X
- Knop FK, Aroda VR, do Vale RD, et al. CagriSema once weekly in adults with overweight or obesity (REDEFINE 1). N Engl J Med. 2025;392(1):22-35. DOI: 10.1056/NEJMoa2412841
- Ahren B, Atkin SL, Charpentier G, et al. Semaglutide induces weight loss in subjects with type 2 diabetes regardless of baseline BMI or gastrointestinal adverse events in the SUSTAIN 1 to 5 trials. Diabetes Obes Metab. 2018;20(9):2210-2219. DOI: 10.1111/dom.13353
- Blonde L, Jendle J, Gross J, et al. Once-weekly dulaglutide versus bedtime insulin glargine, both in combination with prandial insulin lispro, in patients with type 2 diabetes (AWARD-4). Lancet. 2015;385(9982):2057-2066. DOI: 10.1016/S0140-6736(15)60936-9
- Nauck MA, Petrie JR, Sesti G, et al. A phase 2, randomized, dose-finding study of the novel once-weekly human GLP-1 analog, semaglutide, compared with placebo and open-label liraglutide in patients with type 2 diabetes. Diabetes Care. 2016;39(2):231-241. DOI: 10.2337/dc15-0165
- Aroda VR, Rosenstock J, Terauchi Y, et al. PIONEER 1: randomized clinical trial of the efficacy and safety of oral semaglutide monotherapy in comparison with placebo in patients with type 2 diabetes. Diabetes Care. 2019;42(9):1724-1732. DOI: 10.2337/dc19-0749
- Bucheit JD, Pamulapati LG, Carter N, Malloy K, Dixon DL, Sisson EM. Oral semaglutide: a review of the first oral glucagon-like peptide-1 receptor agonist. Diabetes Technol Ther. 2020;22(1):10-18. DOI: 10.1089/dia.2019.0185
- le Roux CW, Zhang S, Riesmeyer JS, et al. Tirzepatide versus semaglutide 2.4 mg once weekly for weight management (SURMOUNT-5). N Engl J Med. 2024;391(18):1732-1742.
- Kadowaki T, Isendahl J, Khalid U, et al. Semaglutide once a week in adults with overweight or obesity, with or without type 2 diabetes in an east Asian population (STEP 6). Lancet Diabetes Endocrinol. 2022;10(3):193-206.
- Lingvay I, Brown-Frandsen K, Colhoun HM, et al. Semaglutide for cardiovascular event reduction in people with overweight or obesity: SELECT study baseline characteristics. Obesity. 2023;31(1):111-122.
- Loomba R, Hartman ML, Lawitz EJ, et al. Tirzepatide for metabolic dysfunction-associated steatohepatitis with liver fibrosis. N Engl J Med. 2024;391(4):299-310.
- Ludvik B, Giorgino F, Jodar E, et al. Once-weekly tirzepatide versus once-daily insulin degludec as add-on to metformin with or without SGLT2 inhibitors in patients with type 2 diabetes (SURPASS-3). Lancet. 2021;398(10300):583-598.
- Bergenstal RM, Wysham C, Macconell L, et al. Efficacy and safety of exenatide once weekly versus sitagliptin or pioglitazone as an adjunct to metformin for treatment of type 2 diabetes (DURATION-2). Lancet. 2010;376(9739):431-439.
- Sattar N, Lee MMY, Kristensen SL, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021;9(10):653-662.
- American Diabetes Association Professional Practice Committee. Pharmacologic approaches to glycemic treatment: Standards of Care in Diabetes - 2026. Diabetes Care. 2026;49(Suppl 1):S181-S218.
- Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22(Suppl 3):1-203.
- Muller TD, Bluher M, Tschop MH, DiMarchi RD. Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov. 2022;21(3):201-223. DOI: 10.1038/s41573-021-00337-8
- Heymsfield SB, Wadden TA. Mechanisms, pathophysiology, and management of obesity. N Engl J Med. 2017;376(3):254-266. DOI: 10.1056/NEJMra1514009
- Rubino F, Nathan DM, Eckel RH, et al. Metabolic surgery in the treatment algorithm for type 2 diabetes: a joint statement by international diabetes organizations. Diabetes Care. 2016;39(6):861-877.
- Amaro A, Sugimoto D, Cusi K. A review of GLP-1 receptor agonist use for the treatment of metabolic dysfunction-associated steatohepatitis (MASH). Diabetes Obes Metab. 2024;26(6):2134-2147.