Direct answer (40-60 words)
For most patients self-injecting compounded tirzepatide, a 31-gauge, 5/16-inch (8 mm) needle on a U-100 insulin syringe is the standard pick. It reaches the subcutaneous layer in average body fat without going into muscle and is thin enough that most patients describe the injection as a pinch rather than a stick.
Table of contents
- The 30-second answer
- Two numbers that matter: gauge and length
- Standard recommendation for compounded tirzepatide
- When to consider 4 mm versus 8 mm versus 1/2-inch
- Syringe barrel sizes (0.3 mL, 0.5 mL, 1 mL)
- Brand pen needles vs insulin syringe needles
- Injection technique that matters more than needle choice
- Pain, bruising, and lumps: troubleshooting
- Sharps disposal and re-use safety
- FAQ
- Footer disclaimers
Two numbers that matter: gauge and length
Every needle has two specifications, and they affect your injection differently.
Check your GLP-1 eligibility
Use our free BMI Calculator to see if you may qualify for provider-reviewed GLP-1 therapy.
Try the BMI Calculator →Gauge. This is the diameter of the needle. Counterintuitively, a higher gauge number means a thinner needle. A 31-gauge needle is finer than a 25-gauge needle. Thinner needles cause less pain, less tissue damage, and slightly slower medication flow. For peptide injections of well under 1 mL, the slow flow doesn't matter.
Length. This is the depth the needle reaches once inserted. Length is measured in either inches or millimeters and is printed on the needle packaging. The two scales overlap: 5/16 inch equals 8 mm, 3/16 inch equals 4-5 mm, and 1/2 inch equals 12.7 mm.
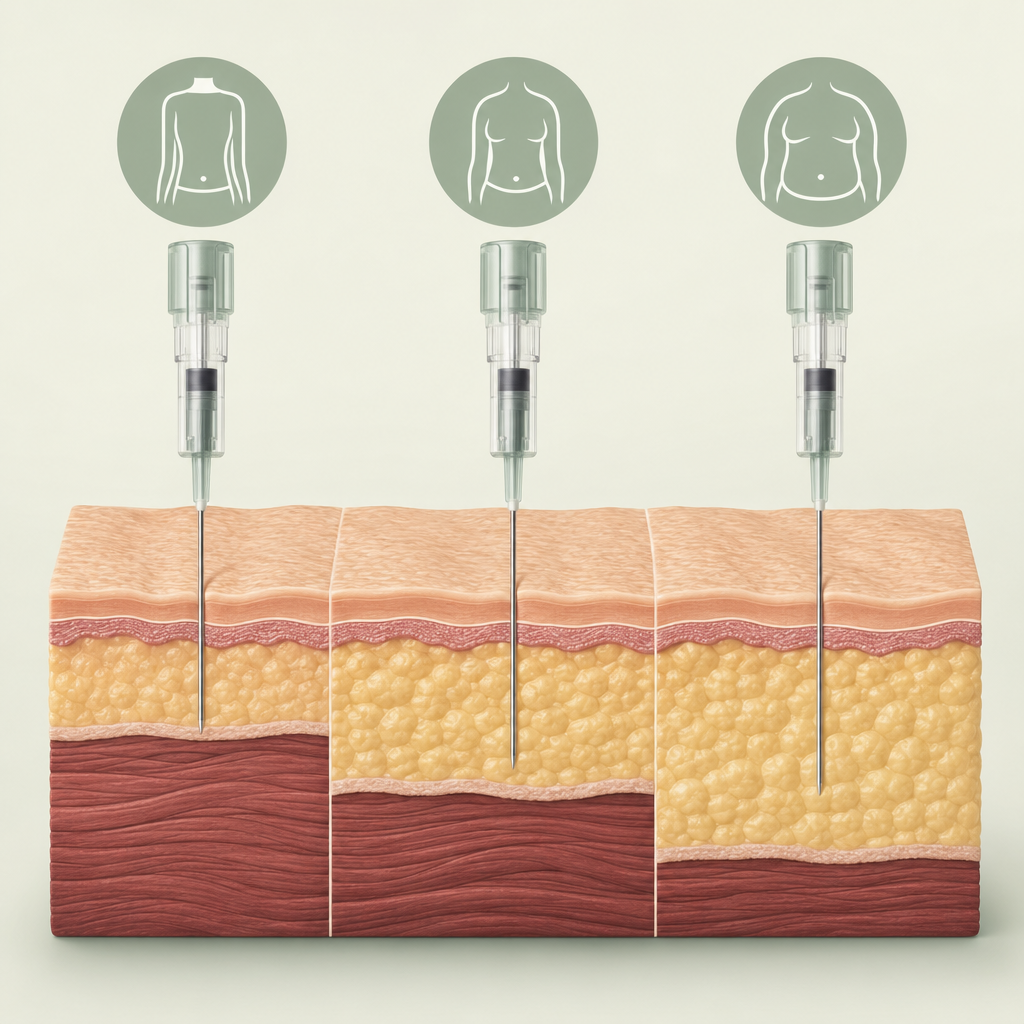
Tirzepatide is a subcutaneous medication. It needs to land in the fat layer between the skin and the muscle. If the needle is too short, the injection ends up intradermal (in the skin layer) and absorption is unpredictable. If the needle is too long, the injection lands in muscle, which absorbs faster than intended and can be more uncomfortable.
The subcutaneous layer thickness varies. The abdomen averages 8 to 25 mm of fat in adults. The thigh averages 5 to 15 mm. The upper arm averages 4 to 12 mm. Most needles for subcutaneous injection are designed to reliably hit the middle of that range without crossing into muscle.
Standard recommendation for compounded tirzepatide
For most patients drawing tirzepatide from a vial with a U-100 insulin syringe, this is the default:
- Gauge: 31 (sometimes 30 or 32 depending on what your pharmacy provides)
- Length: 5/16 inch (8 mm)
- Barrel size: 0.3 mL (for doses under 30 units) or 0.5 mL (for doses 30 to 50 units)
- Syringe type: U-100 insulin syringe with permanently attached needle
This combination works for the majority of adult patients. It reaches the subcutaneous fat in the abdomen, thigh, and upper arm at a 90-degree angle without needing a pinch in patients with average to higher body fat. The 31-gauge thinness means most patients rate the injection at 1-2 out of 10 on a pain scale.
If your pharmacy ships a different default (some send 30-gauge, 5/16-inch, which is also fine, or 31-gauge, 1/2-inch for higher BMI patients), use what they sent unless you have a specific reason to switch.
When to consider 4 mm versus 8 mm versus 1/2-inch
The "standard" 8 mm length is the right pick for most adults, but body composition matters.
4 mm (3/16 inch). Best for very lean patients, especially those with under 8% body fat (rare in this patient population) or for thigh injections in patients with thin upper-leg fat. The 4 mm needle hits subcutaneous tissue at a 90-degree angle without skin pinching, but it can leak medication out of the injection site if not held correctly. Pain is minimal because there's less tissue traversed.
5/16 inch (8 mm). The default for most adult patients. Hits subcutaneous fat reliably across the abdomen and thigh at 90 degrees. Works for patients up to roughly 35 BMI without modification. Above that, the abdomen still works, but the upper arm and thigh may need a pinch-and-inject technique.
1/2 inch (12.7 mm). Used for higher-BMI patients (typically 35+) where the 8 mm length might land too superficially in the abdomen. Also occasionally used for thigh injections in patients with substantial leg adipose tissue. The 1/2-inch length increases the risk of intramuscular injection if not used with a pinch-fold technique.
| Body composition | Recommended length | Technique |
|---|---|---|
| Very lean (BMI under 20) | 4 mm | 90 degrees, no pinch needed |
| Average (BMI 20-30) | 5/16 in (8 mm) | 90 degrees, optional pinch |
| Higher BMI (30-35) | 5/16 in (8 mm) or 1/2 in | 90 degrees with pinch |
| Higher BMI (35+) | 1/2 in (12.7 mm) | Pinch-fold required, 90 degrees |
A 2022 study (Frid et al., Mayo Clinic Proceedings, on subcutaneous injection technique) found that needle length is more often wrong on the long side than the short side. Patients who grew up using insulin pens often default to 1/2-inch needles, which works for insulin but routinely lands tirzepatide in muscle for thinner patients. If you're switching from insulin, reconsider your default.
Syringe barrel sizes (0.3 mL, 0.5 mL, 1 mL)
The barrel size affects how readable the unit markings are.
0.3 mL barrel. Marked in 0.5-unit increments. Holds up to 30 units. Best for tirzepatide doses under 30 units (which covers nearly all maintenance doses up to 7.5 mg at 10 mg/mL). The fine markings make small-dose accuracy much easier.
0.5 mL barrel. Marked in 1-unit increments. Holds up to 50 units. Use this if your dose runs 30 to 50 units (e.g., 10 mg or higher at 10 mg/mL, or any dose at 5 mg/mL).
1 mL barrel. Marked in 2-unit increments on most brands. Holds up to 100 units. Rarely needed for tirzepatide, but useful if your pharmacy uses a 5 mg/mL concentration and your prescribed dose is 12.5 mg or higher (which is 125 units). The wider markings make small-dose accuracy harder.
For most patients on a 10 mg/mL compounded tirzepatide protocol, a 0.3 mL syringe is the right pick from the start of titration through 7.5 mg. Switching to a 0.5 mL once you reach 10 mg or higher.
Brand pen needles vs insulin syringe needles
If you're using brand Mounjaro or Zepbound, you don't pick the needle. The autoinjector pen has a hidden, pre-attached 27 to 29 gauge needle that is engineered to deploy at a fixed depth. There's no choice to make and no parts to swap.
If you're using compounded tirzepatide drawn from a vial, you pick everything. The U-100 insulin syringe and needle ship as one piece in most pharmacy fulfillment, but the gauge and length depend on what your pharmacy stocked. Always check the syringe wrapper before drawing.
The clinical difference: brand pen needles are slightly thicker than what most compounded patients use (29 gauge vs 31 gauge). Patients switching from brand to compounded often comment that the compounded injection feels thinner. That's the gauge change, not the medication.
For dose math on compounded tirzepatide, see our units-to-mg conversion guide and the 60 units of tirzepatide guide.
Injection technique that matters more than needle choice
Patients spend a lot of time picking the perfect needle and not enough on technique. The technique points below affect comfort and absorption more than gauge or length differences within the standard range.
Site rotation. Use a different injection site each week. The pattern most clinicians recommend: abdomen left side week 1, abdomen right side week 2, left thigh week 3, right thigh week 4, repeat. This prevents lipohypertrophy (fatty tissue thickening that reduces absorption) and lets each site recover.
Avoid the navel zone. The 2-inch ring around the belly button has different vascular and connective tissue properties. Injections there are more likely to bruise and have variable absorption.
Wait for alcohol to dry. Wet alcohol on the skin gets carried into the injection site by the needle and produces a sting that gets blamed on the medication. Let the alcohol swab evaporate fully (15 to 20 seconds) before injecting.
Bring the medication to room temperature. Injecting cold medication straight from the fridge causes a noticeable burn. Take the vial out 15 to 30 minutes before drawing your dose, or warm it in your hand briefly. Don't microwave or heat above room temperature.
Inject perpendicular at 90 degrees. A 45-degree angle is occasionally recommended for very lean patients with 4 mm needles, but for the standard 5/16-inch needle, 90 degrees with or without a pinch is correct. Slanted insertion can land in dermis or muscle.
Push slow, hold for 5 seconds. A slow push reduces tissue trauma and the burning sensation. Holding the needle in for 5 seconds after the plunger bottoms out lets the medication disperse into surrounding tissue rather than tracking back along the needle path when you withdraw.
Pain, bruising, and lumps: troubleshooting
Sharp pain at insertion. Usually a needle dulled by going through the rubber stopper plus the skin. Use a fresh needle if your pharmacy ships syringes with detachable needles. Most pharmacies ship integrated needles where you can't change it. In that case, picking a slightly different injection site usually solves it.
Bruising at the injection site. Common, harmless, and more likely if you're on aspirin, fish oil, or anticoagulants. Avoid pressing hard on the site immediately after withdrawal. Apply gentle pressure with a clean tissue if there's any bleeding, but don't rub.
A small lump under the skin afterward. Usually a temporary depot of medication that hasn't fully absorbed. Resolves within 24 to 48 hours. If a lump persists more than a week, doesn't shrink, or becomes warm or red, contact your provider. Could be lipohypertrophy or, rarely, infection.
Stinging during injection. Usually the medication itself, especially if it was cold or the alcohol wasn't dry. Stinging that lasts longer than a few seconds after the injection ends or radiates beyond the site warrants a call to your provider.
Persistent itching at the site. Could be a local hypersensitivity reaction. Common in the first few weeks, usually resolves. If itching is severe, spreads beyond the site, or comes with hives or breathing difficulty, treat it as a possible allergic reaction and seek immediate medical attention.
Sharps disposal and re-use safety
Used insulin syringes are sharps and should never go in regular trash. The medical-grade options:
- A purchased FDA-cleared sharps container, available at most pharmacies for $5 to $15.
- A sturdy household container with a screw-on lid (a heavy-duty laundry detergent bottle works) labeled "SHARPS" in marker. Tape the lid when full.
- A sharps mail-back program. Several companies offer prepaid containers.
Don't put used syringes loose in trash bags. Sanitation workers are routinely injured by improperly disposed sharps. Many cities have free drop-off at municipal collection sites.
Never reuse a needle. Single-use means single-use. Even if a syringe looks clean, the needle bevel dulls after one pass through skin, and re-use increases pain, tissue damage, and infection risk. The cost savings of re-use is not worth the clinical risk.
FAQ
What size needle is best for tirzepatide?
For most adult patients self-injecting compounded tirzepatide, a 31-gauge, 5/16-inch (8 mm) needle on a U-100 insulin syringe is the default. Higher BMI patients (35+) sometimes need 1/2-inch length. Very lean patients can use 4 mm.
Is a smaller-gauge needle better?
A higher gauge number means a thinner needle, which is less painful. 31 to 32 gauge is the comfort range for tirzepatide. Going below 30 gauge offers no benefit and increases discomfort.
Can I use a regular syringe instead of an insulin syringe?
No. Regular syringes are calibrated in milliliters with markings too coarse for tirzepatide doses. A 1 mL standard syringe might be marked in 0.1 mL increments, which is 10 units of error. Use a U-100 insulin syringe with unit markings.
What gauge does a Mounjaro or Zepbound pen use?
The brand pens have integrated 27 to 29 gauge needles that you can't change. The pen handles depth and gauge automatically. You don't pick the needle.
Should I use a 4 mm or 5/16 inch needle?
For most adults, 5/16 inch (8 mm) is the default. 4 mm is appropriate for very lean patients or for thigh injections in patients with thin leg fat. Discuss with your provider if uncertain.
Does needle size affect tirzepatide absorption?
If the needle reaches subcutaneous fat correctly, absorption is consistent. A needle too short for your body composition can land intradermal and produce unpredictable absorption. A needle too long can land intramuscular and absorb faster than intended.
Can I switch needle sizes without telling my provider?
For routine size changes within standard ranges (4 mm to 5/16 inch), most providers don't require notification. If you're considering a 1/2-inch needle because of BMI, mention it at your next check-in. The clinical difference is small but worth confirming.
How do I know if my needle is too long?
Signs include sharper pain than usual, a sensation of hitting a hard layer (muscle), faster onset of side effects after injection, and bruising deeper than the skin level. A switch to a shorter needle usually resolves these.
Can I reuse an insulin syringe?
No. Single-use only. Even if it looks clean, the needle bevel dulls after one use, increasing pain and infection risk. Used syringes go in a sharps container.
Are 30-gauge and 31-gauge needles interchangeable?
Functionally, yes. The diameter difference is small enough that most patients can't tell. If your pharmacy ships 30-gauge by default, no reason to switch. If they ship 31-gauge, also fine. Both are standard for compounded GLP-1 use.
Does the needle length change with the injection site?
Sort of. The 5/16-inch needle works at the abdomen for most BMIs and works at the thigh for average to higher body fat. For thigh injections in lean patients, a 4 mm needle is sometimes preferred. The arm rarely needs a different needle than the abdomen.
How often should I change to a new needle?
Every injection. Used needles are dull, contaminated, and unsafe to reuse. Every weekly injection gets a fresh syringe and needle.
Author / review note
Reviewed by the FormBlends Medical Team. References include Frid AH et al., Mayo Clinic Proceedings, 2022 (FITTER recommendations on subcutaneous injection technique), the U.S. Pharmacopeia chapter on insulin syringes (USP <797>), and ISO 11608-1 / ISO 8537 standards for needle dimensions and labeling. The CDC sharps disposal guidance was also referenced for the disposal section.
Footer disclaimers
Platform Disclaimer. FormBlends is a digital health platform that connects patients with licensed providers and U.S.-based pharmacies. We do not manufacture, prescribe, or dispense medication directly. All clinical decisions are made by independent licensed providers.
Compounded Medication Notice. Compounded semaglutide and tirzepatide are not FDA-approved. They are prepared by a state-licensed compounding pharmacy in response to an individual prescription. Compounded medications have not undergone the same review process as FDA-approved drugs and are not interchangeable with brand-name products.
Results Disclaimer. Individual results vary. Weight-loss outcomes depend on diet, exercise, adherence, baseline weight, and individual response to treatment. Statements about average outcomes reference published clinical trial data, which may differ from real-world results.
Trademark Notice. Mounjaro and Zepbound are registered trademarks of Eli Lilly and Company. FormBlends is not affiliated with, endorsed by, or sponsored by Eli Lilly. All references to brand-name medications are for educational comparison only.
Related guides
- What Size Needle for Tirzepatide? The Complete Gauge and Length Guide for Compounded Vials
- What Needle Size Does Zepbound Use? Auto-Injector and Compounded Tirzepatide Comparison
- How to Avoid Gastroparesis on Mounjaro: A Practical Protocol for Safer Tirzepatide Use
- What Happens If Tirzepatide Gets Warm? A Practical Storage and Stability Guide
- Can You Take Berberine With Tirzepatide? Mechanisms, Risks, and a Practical Protocol
- What Happens If You Inject Tirzepatide Into Muscle Instead of Fat? The Pharmacokinetic and Practical Effects
See your options in about 2 minutes
Take the free quiz and see what fits you. Quick, private, and no commitment to continue.
See my options →