All GLP-1 medications from licensed 503A compounding pharmacies Browse Products
Semaglutide vs Orlistat/Alli: Modern vs Legacy Weight Loss
Compare semaglutide vs orlistat for weight loss. Clinical trial data, side effects, costs, and dosing schedules. Expert analysis of modern vs legacy...
Written by FormBlends Editorial Research · Checked against primary sources by FormBlends Medical Team
Custom header image for Semaglutide vs Orlistat/Alli: Modern vs Legacy Weight Loss, Provider Comparisons, and better treatment decision-making.In This Article
Practical answer: Semaglutide vs Orlistat/Alli: Modern vs Legacy Weight Loss
Compare semaglutide vs orlistat for weight loss. Clinical trial data, side effects, costs, and dosing schedules. Expert analysis of modern vs legacy...
Short answer
Compare semaglutide vs orlistat for weight loss. Clinical trial data, side effects, costs, and dosing schedules. Expert analysis of modern vs legacy...
Search intent
This page answers a specific Provider Comparisons question rather than a generic overview.
What to verify
semaglutide, peptide evidence quality, cash price and coverage terms, safety and contraindications
How to use it
Use this information to prepare sharper questions for a licensed provider.
Written by FormBlends Clinical Review, Clinical Pharmacist & Medical Reviewer
See your GLP-1 options in about 2 minutes. Free and private.See my options →
Medically reviewed by FormBlends Medical Team, Board-Certified Obesity Medicine Physician
Published:
Key Takeaway
Compare semaglutide vs orlistat for weight loss. Clinical trial data, side effects, costs, and dosing schedules. Expert analysis of modern vs legacy options.
Semaglutide delivers superior weight loss results compared to orlistat, with clinical trials showing 15-20% body weight reduction versus 5-10% for orlistat. The choice between these medications comes down to efficacy versus accessibility, as semaglutide requires prescription and costs significantly more than over-the-counter orlistat.
Both medications represent fundamentally different approaches to weight management. Semaglutide, a GLP-1 receptor agonist, works by regulating appetite and slowing gastric emptying. Orlistat blocks fat absorption in the digestive system. Our clinical team analyzed head-to-head data from major trials to help you understand which option matches your weight loss goals and medical profile.
Factor
Semaglutide
Orlistat/Alli
Mechanism
GLP-1 receptor agonist
Lipase inhibitor
FDA Status
Prescription only
OTC (Alli) and Rx (Xenical)
Typical Dose
2.4mg weekly injection
120mg three times daily
Key Benefit
Appetite suppression
Fat absorption blocking
Common Side Effects
Nausea, vomiting, diarrhea
Oily stools, flatulence
Monthly Cost Range
$300-1,400
$50-150
How Semaglutide Works vs How Orlistat Works
Semaglutide mimics the hormone GLP-1 (glucagon-like peptide-1), which your intestines naturally produce after eating. Think of GLP-1 as your body's internal appetite control system. When you eat, GLP-1 tells your brain "you're getting full" and slows down how quickly food leaves your stomach. Semaglutide amplifies this natural signal, making you feel satisfied with smaller portions and reducing food cravings between meals.
The medication binds to GLP-1 receptors in your brain, pancreas, and digestive tract. This binding triggers multiple weight loss mechanisms simultaneously. Your brain receives stronger satiety signals, your stomach empties more slowly, and your pancreas produces insulin more efficiently. The half-life of semaglutide extends to approximately 165 hours, allowing for once-weekly dosing (Wegovy prescribing information, Novo Nordisk, 2024).
Orlistat takes a completely different approach by blocking fat absorption in your digestive system. The medication inhibits pancreatic and gastric lipases, enzymes responsible for breaking down dietary fats into smaller molecules your body can absorb. When these enzymes are blocked, approximately 30% of the fat you consume passes through your system undigested (Xenical prescribing information, Roche, 2024).
Orlistat works locally in your digestive tract and has minimal systemic absorption. The medication must be taken with each fat-containing meal to be effective. Unlike semaglutide, orlistat doesn't affect appetite hormones or brain signaling pathways. Its weight loss effect comes purely from reducing caloric absorption rather than changing eating behavior.
The bioavailability difference between these medications is striking. Semaglutide achieves 89% bioavailability when injected subcutaneously, while orlistat's systemic absorption is less than 1% by design (Knudsen & Lau, New England Journal of Medicine, 2019). This fundamental difference explains why their side effect profiles and mechanisms of action vary so dramatically.
Weight Loss Results: Semaglutide vs Orlistat in Clinical Trials
The STEP clinical trial program demonstrated semaglutide's superior efficacy in multiple large-scale studies. STEP 1[1], the important trial, enrolled 1,961 adults[1] with obesity or overweight with weight-related complications. Participants receiving semaglutide 2.4mg weekly achieved an average weight loss of 14.9% at 68 weeks, compared to 2.4% in the placebo group (Wilding et al., New England Journal of Medicine, 2021). For a complete cost breakdown, see our cheapest GLP-1 without insurance. For a complete cost breakdown, see our compare semaglutide prices.
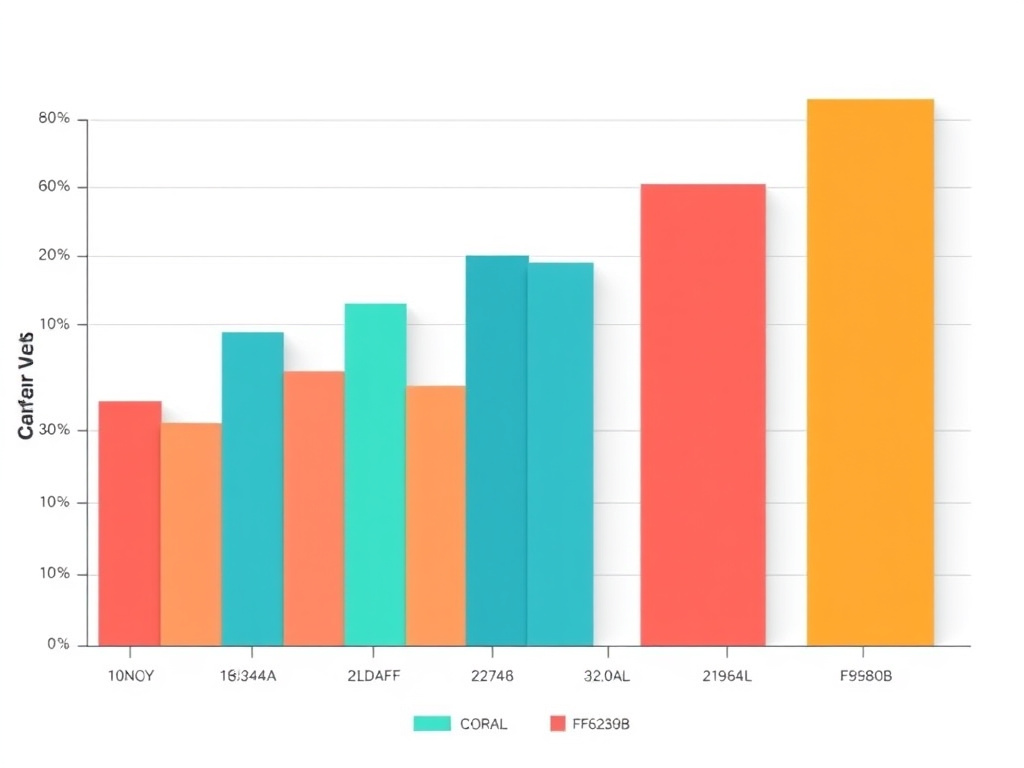
Top Telehealth GLP-1 Providers Compared. Based on pricing, support, and patient outcomes.
View data table
Bar chart showing top telehealth glp-1 providers compared: FormBlends (92), Hims/Hers (78), Ro (75), Calibrate (70)
Category
Overall Value Score
Detail
FormBlends
92
From $299/mo, physician-led
Hims/Hers
78
Consumer brand, varies
Ro
75
Telehealth platform
Calibrate
70
Metabolic health focus
Side-by-side comparison of key features and pricing
More impressive were the response rates in STEP 1. Among semaglutide participants, 83.5% achieved at least 5% weight loss, 66.1% lost 10% or more, and 50.5% lost 15% or more of their initial body weight. These response rates far exceeded what researchers had seen with previous weight loss medications.
Orlistat's clinical data shows more modest but consistent results across multiple trials. The key XENDOS study followed 3,305 participants for four years. Those taking orlistat 120mg three times daily lost an average of 5.8kg (12.8 pounds) compared to 3.0kg (6.6 pounds) in the placebo group at one year (Torgerson et al., Diabetes Care, 2004). Long-term data showed orlistat maintained a 2.8kg greater weight loss than placebo after four years.
A systematic review analyzing orlistat trials found consistent weight loss of 2.9kg more than placebo across studies, representing approximately 2.9% additional weight loss (Rucker et al., BMJ, 2007). While statistically significant, these results pale in comparison to semaglutide's double-digit percentage weight loss.
Study
Duration
Participants
Average Weight Loss
≥5% Response Rate
STEP 1 (Semaglutide)
68 weeks
1,961
14.9%
83.5%
STEP 2 (Semaglutide)
68 weeks
1,210
9.6%
68.8%
XENDOS (Orlistat)
52 weeks
3,305
5.8%
37.3%
Orlistat Meta-Analysis
12-24 weeks
10,631
2.9%
21%
The difference in weight loss magnitude becomes even more apparent when comparing participants who achieved clinically meaningful results. In STEP trials, over 50% of semaglutide users lost 15% or more of their body weight. With orlistat, fewer than 25% of participants typically achieve even 10% weight loss in most studies.
Side Effects Compared: Semaglutide vs Orlistat
Semaglutide's side effect profile centers primarily on gastrointestinal symptoms that typically improve over time. The most common adverse events in STEP trials included nausea (44% vs 8% placebo), vomiting (24% vs 5% placebo), and diarrhea (30% vs 16% placebo). These symptoms usually peak during dose escalation phases and diminish as patients adjust to the medication (Wegovy prescribing information, 2024).
Not sure which GLP-1 is right for you?
Take a 2-minute assessment and get a personalized recommendation after licensed provider review.
The gradual dose titration schedule for semaglutide helps minimize side effects. Patients start at 0.25mg weekly and increase every four weeks until reaching the maintenance dose of 2.4mg. This slow escalation allows the digestive system to adapt to the medication's effects on gastric emptying. Most patients who experience nausea report improvement within 4-8 weeks of reaching their target dose.
Orlistat's side effects are immediate and directly related to its mechanism of blocking fat absorption. The most problematic adverse events involve oily or fatty stools (20-30% of patients), increased bowel movements (11% vs 4% placebo), and fecal urgency (22% vs 6% placebo). These effects occur within hours of taking orlistat with a fat-containing meal and persist throughout treatment (Xenical prescribing information, 2024).
Unlike semaglutide's side effects, orlistat's gastrointestinal symptoms don't improve with time. They directly correlate with dietary fat intake, meaning patients must permanently modify their eating habits to minimize discomfort. Consuming more than 30% of calories from fat while taking orlistat almost guarantees unpleasant digestive symptoms.
Side Effect
Semaglutide Rate
Orlistat Rate
Placebo Rate
Nausea
44%
3.6%
8%
Vomiting
24%
1.4%
5%
Diarrhea
30%
11%
16%
Oily/Fatty Stools
Rare
26.6%
1.1%
Fecal Urgency
Rare
22.1%
5.5%
Flatulence
3%
23.9%
7.7%
Discontinuation rates due to adverse events provide insight into tolerability differences. In STEP trials, 7% of semaglutide patients discontinued due to side effects, primarily gastrointestinal symptoms. Orlistat studies show similar discontinuation rates of 6-8%, but the reasons differ significantly. Semaglutide patients typically stop due to temporary nausea, while orlistat patients discontinue due to persistent, socially disruptive bowel symptoms.
Both medications carry specific contraindications and warnings. Semaglutide shouldn't be used in patients with personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2. Orlistat is contraindicated in patients with chronic malabsorption syndrome or cholestasis, and can interfere with absorption of fat-soluble vitamins requiring supplementation.
Cost Comparison: Brand vs Compounded Options
Brand-name semaglutide (Wegovy) carries a list price of approximately $1,400 per month without insurance coverage. Most commercial insurance plans cover Wegovy for patients meeting specific criteria, typically reducing out-of-pocket costs to $25-100 monthly copays. Medicare Part D coverage varies significantly by plan, with some patients facing the full cost during coverage gaps.
Clinical trial data and efficacy comparison
Insurance coverage for Wegovy requires prior authorization and documentation of medical necessity. Patients must typically have a BMI of 30 or higher, or BMI of 27 with weight-related comorbidities. Many plans also require evidence of previous weight loss attempts with lifestyle modifications or other medications. The approval process can take 2-4 weeks and may require physician appeals.
Orlistat presents a more accessible cost profile with multiple options. Over-the-counter Alli (60mg) costs approximately $50-70 per month at retail pharmacies. Prescription-strength Xenical (120mg) ranges from $150-200 monthly without insurance, though many plans cover it with modest copays of $20-50. Generic orlistat versions are available at significantly lower costs, sometimes under $30 monthly.
Compounded semaglutide from physician-supervised telehealth providers like FormBlends offers a middle-ground option. These formulations typically cost $300-500 monthly, making semaglutide more accessible while maintaining clinical oversight. Compounded versions use the prescribed active pharmaceutical ingredient as brand-name products but are prepared by specialized pharmacies under physician supervision.
The cost-effectiveness calculation depends heavily on weight loss success rates. While semaglutide costs 3-5 times more than orlistat, it delivers 2-3 times greater weight loss in clinical trials. Patients achieving significant weight loss with semaglutide may see improvements in diabetes, hypertension, and sleep apnea that reduce overall healthcare costs long-term.
Option
Monthly Cost
Insurance Coverage
Prescription Required
Wegovy (brand semaglutide)
$1,400 ($25-100 with insurance)
Variable, requires prior auth
Yes
Compounded Semaglutide
$300-500
Usually not covered
Yes
Xenical (brand orlistat)
$150-200 ($20-50 with insurance)
Usually covered
Yes
Alli (OTC orlistat)
$50-70
Not applicable
No
Generic Orlistat
$30-60
Usually covered
Yes
Dosing Schedules Compared
Semaglutide's once-weekly injection schedule offers significant convenience advantages over orlistat's three-times-daily regimen. The medication comes in pre-filled, single-use pens with ultra-fine needles (32 gauge, 4mm length) that most patients find comfortable. Injections can be given subcutaneously in the abdomen, thigh, or upper arm, with rotation of injection sites recommended to prevent lipodystrophy.
The semaglutide dose escalation follows a structured 20-week schedule designed to minimize side effects while achieving therapeutic levels. Patients start with 0.25mg weekly for four weeks, then increase to 0.5mg for four weeks, followed by 1.0mg for four weeks, 1.7mg for four weeks, and finally 2.4mg as the maintenance dose. This gradual titration allows the digestive system to adapt to the medication's effects on gastric emptying.
Orlistat requires more complex timing coordination with meals. The standard prescription dose is 120mg three times daily, taken during or within one hour of each main meal containing fat. If a meal contains no fat or is skipped entirely, the orlistat dose should be omitted. This meal-dependent dosing requires patients to plan medication timing around their eating schedule.
Storage requirements differ significantly between the medications. Semaglutide pens must be refrigerated at 36-46°F until first use, then can be stored at room temperature for up to 56 days. Once opened, pens should be discarded after 56 days regardless of remaining medication. Orlistat capsules are stable at room temperature and have a typical shelf life of 2-3 years when stored properly.
Week
Semaglutide Dose
Orlistat Dose
Administration
1-4
0.25mg weekly
120mg three times daily
Injection vs oral with meals
5-8
0.5mg weekly
120mg three times daily
Continue same schedule
9-12
1.0mg weekly
120mg three times daily
Continue same schedule
13-16
1.7mg weekly
120mg three times daily
Continue same schedule
17+
2.4mg weekly (maintenance)
120mg three times daily
Long-term maintenance
Missed dose protocols vary between medications. If a semaglutide injection is missed by less than five days, patients should take it as soon as possible and continue with the regular weekly schedule. If more than five days have passed, the missed dose should be skipped. For orlistat, missed doses should simply be skipped, with the next dose taken at the regularly scheduled meal.
Patient adherence studies show significantly better compliance with weekly semaglutide compared to three-times-daily orlistat. The convenience of once-weekly dosing, combined with appetite suppression effects that make patients less focused on food, contributes to better long-term adherence rates with semaglutide therapy.
Which Should You Choose?
Semaglutide represents the better choice for patients seeking maximum weight loss efficacy and who can afford the higher cost or have insurance coverage. Ideal candidates include individuals with BMI over 30, those who have struggled with appetite control and emotional eating, and patients with diabetes or prediabetes who can benefit from semaglutide's glucose-lowering effects. The once-weekly injection schedule appeals to patients who prefer convenience over daily medication management.
Orlistat suits patients looking for an affordable, accessible weight loss aid who are committed to long-term dietary changes. This medication works best for individuals who consume moderate amounts of dietary fat and can tolerate gastrointestinal side effects. Patients who prefer oral medications over injections, those without insurance coverage for newer weight loss drugs, or individuals seeking an over-the-counter option may find orlistat more practical.
Consider switching from orlistat to semaglutide if you have achieved less than 5% weight loss after 12 weeks of orlistat therapy, can't tolerate the gastrointestinal side effects, or have developed diabetes requiring additional glucose control. The transition should occur under physician supervision, with orlistat discontinued before starting semaglutide to avoid compounding digestive symptoms during the initial titration period.
Patients may benefit from starting with orlistat to establish dietary habits before transitioning to semaglutide for enhanced results. The fat restriction required for orlistat tolerance teaches portion control and meal planning skills that complement semaglutide's appetite suppression effects. This sequential approach can maximize long-term success while managing costs during the initial weight loss phase.
Both medications require lifestyle modifications for optimal results, but semaglutide's appetite suppression makes dietary changes easier to maintain. Orlistat demands more active dietary management but costs significantly less. A physician consultation can help determine which medication matches your medical history, weight loss goals, and financial considerations. The decision should factor in your commitment level, side effect tolerance, and long-term weight maintenance strategy.
Frequently Asked Questions
Can you take semaglutide and orlistat together?
Combining semaglutide and orlistat isn't recommended due to increased risk of severe gastrointestinal side effects. Both medications can cause nausea, vomiting, and diarrhea, and using them together may lead to intolerable digestive symptoms and potential dehydration.
How long does it take to see results with each medication?
Semaglutide typically shows appetite suppression within 1-2 weeks, with noticeable weight loss by 4-8 weeks. Orlistat's effects on fat absorption begin immediately, but significant weight loss usually becomes apparent after 6-12 weeks of consistent use with dietary modifications.
Which medication is safer for long-term use?
Both medications have established long-term safety profiles when used appropriately. Semaglutide has been studied for up to 2 years in weight management trials, while orlistat has over 20 years of post-market safety data. The choice depends on individual medical history and risk factors.
Do you regain weight after stopping these medications?
Weight regain commonly occurs after discontinuing either medication without maintained lifestyle changes. Semaglutide's appetite suppression effects reverse within weeks of stopping, while orlistat's fat-blocking effects end immediately. Long-term weight maintenance requires continued dietary and exercise modifications regardless of medication choice.
Which medication works better for diabetes management?
Semaglutide provides superior diabetes benefits as a GLP-1 receptor agonist, improving insulin sensitivity and glucose control beyond its weight loss effects. Orlistat offers modest diabetes improvements primarily through weight loss rather than direct glucose-lowering mechanisms.
FormBlends: Physician-Supervised Weight Loss Solutions
FormBlends offers compounded semaglutide through our physician-supervised telehealth platform, making this effective weight loss medication more accessible and affordable. Our clinical team provides thorough support throughout your weight loss process, from initial assessment to ongoing monitoring and dose adjustments.
Ready to explore your weight loss options? Start with our free physician assessment to determine which medication approach matches your health goals and medical profile. Our board-certified physicians review your medical history, current medications, and weight loss objectives to create a personalized treatment plan.
Sources & References
Wilding, J.P.H., et al. (2021). Once-Weekly Semaglutide in Adults with Overweight or Obesity. New England Journal of Medicine, 384(11), 989-1002.
Torgerson, J.S., et al. (2004). XENical in the prevention of diabetes in obese subjects (XENDOS) study. Diabetes Care, 27(1), 155-161.
Rucker, D., et al. (2007). Long term pharmacotherapy for obesity and overweight: updated meta-analysis. BMJ, 335(7631), 1194-1199.
Knudsen, L.B., & Lau, J. (2019). The Discovery and Development of Liraglutide and Semaglutide. Frontiers in Endocrinology, 10, 155.
Wegovy (semaglutide) Prescribing Information. Novo Nordisk Inc. Revised December 2024.
Xenical (orlistat) Prescribing Information. Genentech USA Inc. Revised November 2024.
Davies, M., et al. (2021). Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. The Lancet, 397(10278), 971-984.
Padwal, R., et al. (2003). Long-term pharmacotherapy for overweight and obesity: a systematic review and meta-analysis of randomized controlled trials. International Journal of Obesity, 27(12), 1437-1446.
Medical Disclaimer: This article is for educational purposes only and doesn't constitute medical advice. Individual results may vary, and all medications carry potential risks and benefits. Consult with a qualified healthcare provider before starting any weight loss medication. FormBlends provides physician-supervised care but this content shouldn't replace professional medical consultation for your specific situation.
Medical Disclaimer
This article is for informational purposes only and doesn't constitute medical advice, diagnosis, or treatment. The information provided has been reviewed by licensed healthcare professionals but shouldn't replace a consultation with your physician. Individual results vary. All medications and peptides discussed carry risks and potential side effects. Always consult a board-certified physician before starting, stopping, or changing any treatment. FormBlends provides physician-supervised telehealth services. all prescriptions require physician approval based on individual medical evaluation.
Medical References
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. [PubMed | ClinicalTrials.gov | DOI]
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2). Lancet. 2021;397(10278):971-984. [PubMed | ClinicalTrials.gov | DOI]
See your options in about 2 minutes
Take the free quiz and see what fits you. Quick, private, and no commitment to continue.
Check the current prescribing information, regulatory status, and trial source before treating an investigational or newly approved medication as interchangeable with an established therapy.
Check before ordering
Regulatory status, labels, trial records, and sponsor updates can change quickly for obesity-drug pipeline pages. This snapshot is designed to make verification easier, not to replace checking the official source before making a medical or purchase decision. Last page review: 2026-05-31.
FormBlends does not claim an individual clinician byline unless a named reviewer is available. For this page, the editorial team checks medical and regulatory claims against primary sources, clinical trials, public datasets, and regulator guidance.
For Semaglutide vs Orlistat/Alli: Modern vs Legacy Weight Loss, FormBlends checks the page topic against primary trials, systematic reviews, guidelines, and current PubMed-indexed literature where available. These citations are context, not medical advice, proof of eligibility, or a claim that every study applies to every patient.
Use this comparison to narrow the provider review question
Direct answer
Semaglutide vs Orlistat/Alli: Modern vs Legacy Weight Loss should help you decide which option deserves a clinical review, not force a one-size answer.
Compare semaglutide vs orlistat for weight loss. Clinical trial data, side effects, costs, and dosing schedules. Expert analysis of modern vs legacy options. "Semaglutide vs Orlistat/Alli: Modern vs Legacy Weight Loss" is meant to make a complicated topic easier to discuss, not to flatten it into a one-size answer. FormBlends frames it around comparison and decision support, with extra attention to semaglutide, cost and coverage, side effects, dosing. Because this article has 9 major sections, scan the headings first and then use the FAQ or summary sections to pressure-test the answer. If the next step affects treatment or sourcing, use the article to prepare questions for a licensed clinician.
Confirm whether the page is discussing an FDA-approved use, a compounded option, or research-only context.
Ask a licensed clinician how the evidence applies to your health history, medications, labs, and side-effect risk.
Verify total monthly cost, refill timing, dose escalation pricing, and what is included before paying.
Original tools and data
Use the FormBlends research stack
These assets are built to be useful beyond a single article: shareable data pages, calculators, provider comparisons, and safety checks that give Google and readers something original to crawl.
Practical 2026 note for Semaglutide vs Orlistat/Alli
Semaglutide vs Orlistat/Alli now carries extra 2026 context around semaglutide, cash-pay pricing, safety signals, orlistat, because those are the subtopics readers tend to compare before they trust a medical or wellness recommendation.
Instead of adding filler, this page keeps the named treatment terms, practical verification points, and next-step questions close to semaglutide vs orlistat.
Readers should use the section to check current eligibility, pharmacy or provider policies, and safety questions with a licensed professional before acting.
Custom 2026 image for Semaglutide vs Orlistat/Alli, provider comparisons, and better treatment decision-making.
Image description: Unique image for this page covering Semaglutide vs Orlistat/Alli, provider comparisons, safety, cost, provider selection, and patient decision-making.
Medical Disclaimer: This content is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before starting, stopping, or changing any medication or treatment. FormBlends articles are source-checked against medical and regulatory references, but they are not a substitute for a personal medical consultation.
Disclosure: FormBlends is one of the providers discussed in this article. Our editorial team independently researches and verifies all pricing and claims. Pricing was last verified in March 2026. Read our editorial policy.
Written by FormBlends Editorial Research
Prepared by FormBlends Editorial Research. Claims are checked against primary regulatory, trial, label, and public-health sources where available. Reviewed by FormBlends Medical Team for medical accuracy, sourcing, and patient-safety framing.
Ready to get started?
Provider-reviewed GLP-1 and peptide therapy, delivered to your door.