Executive Summary
Key Takeaways
- Figure 1: Body composition during GLP-1 therapy requires active management to preserve lean tissue while maximizing fat loss.
- GLP-1 receptor agonists produce dramatic weight loss, but 25-40% of the weight shed comes from lean tissue rather than fat.
- The numbers are clear and, for many patients, alarming.
- When someone loses 15% of their body weight on semaglutide, roughly 5-6% of that total comes from lean mass rather than adipose tissue.
- In absolute terms, a person who drops 35 pounds might lose 10-14 pounds of muscle, bone mineral, and organ tissue.
GLP-1 receptor agonists produce dramatic weight loss, but 25-40% of the weight shed comes from lean tissue rather than fat. This report quantifies that muscle loss across every major clinical trial, then provides actionable protocols to minimize it.
The numbers are clear and, for many patients, alarming. When someone loses 15% of their body weight on semaglutide, roughly 5-6% of that total comes from lean mass rather than adipose tissue. In absolute terms, a person who drops 35 pounds might lose 10-14 pounds of muscle, bone mineral, and organ tissue. That's not a trivial amount. For older adults already at risk of sarcopenia, or for anyone who values physical performance, those numbers demand attention.
But here's what rarely gets discussed in the headlines: muscle loss during pharmacological weight loss isn't inevitable at these ratios. It's largely preventable. The research on resistance training, protein optimization, and adjunctive therapies shows that you can slash the lean mass fraction of weight loss by half or more with the right interventions. The problem isn't that solutions don't exist. It's that most prescribers don't emphasize them, and most patients don't know they're necessary.
What This Report Covers
We'll walk through every major body composition study from the STEP, SURMOUNT, SUSTAIN, and SCALE trial programs. You'll see exactly how much lean mass was lost in each, how the numbers compare between semaglutide and tirzepatide, and what factors predict who loses more muscle versus less. Then we shift to solutions.
The prevention sections cover protein targets with specific gram-per-kilogram recommendations, resistance training protocols with set and rep ranges, supplement strategies centered on creatine monohydrate, and combination approaches using peptides like CJC-1295/Ipamorelin and MK-677 that support growth hormone pathways. We also address the phenomenon colloquially known as "Ozempic face" and why it's distinct from true sarcopenia.
Why Lean Mass Matters More Than Scale Weight
Skeletal muscle isn't just for aesthetics. It's the body's largest glucose disposal organ, the primary driver of resting metabolic rate, and a critical reservoir for amino acids during illness or stress. Every pound of lean tissue burns approximately 6-10 calories per day at rest, compared to about 2 calories per pound of fat tissue. Lose 10 pounds of muscle and your daily energy expenditure drops by 60-100 calories, creating a metabolic environment that practically invites weight regain.
There's also the functional dimension. Grip strength, walking speed, and the ability to rise from a chair without assistance all correlate with skeletal muscle mass. For adults over 60, losing substantial lean tissue during weight loss can push them across the threshold from functional independence to disability. The GLP-1 research hub tracks emerging data on long-term functional outcomes, but the existing evidence already points in a concerning direction for patients who lose weight without muscle-protective interventions.
The Scale of the Problem
An estimated 25 million Americans will be using GLP-1 receptor agonists by 2027, according to Goldman Sachs projections. If even half of those patients lose meaningful lean mass without adequate prevention, we're looking at a population-level decline in metabolic health and physical function. The irony would be striking: drugs prescribed to improve metabolic health inadvertently contributing to sarcopenic obesity when patients regain weight but not muscle.
This isn't hypothetical. The STEP 1 extension data already showed that patients who discontinued semaglutide regained roughly two-thirds of their lost weight within a year, but body composition analysis suggested the regained weight was disproportionately fat rather than lean tissue. You end up with a worse body composition than where you started. Our weight loss mechanisms report covers the pharmacological basis for this pattern.
KEY TAKEAWAY
GLP-1 drugs are highly effective for fat loss, but without concurrent resistance training and adequate protein intake, 25-40% of weight lost comes from lean tissue. Simple, evidence-based interventions can cut that ratio to 15-20% while preserving the metabolic benefits of weight loss.
A Practical Framework
Every section that follows is built around actionable recommendations. We don't just quantify the problem; we provide specific protocols you can implement immediately. Whether you're a clinician counseling patients, a patient starting tirzepatide, or a researcher studying body composition, you'll find data-driven guidance throughout.
The core message is simple: GLP-1-mediated weight loss produces the best outcomes when it's combined with structured resistance exercise, optimized protein intake, and, where appropriate, peptide-based growth hormone support. The drugs handle the appetite and caloric side. Your job is to protect the muscle. Let's look at exactly how to do that.
For a broader perspective on all GLP-1 side effects and management strategies, see our complete side effects guide. And for those exploring their options across the full GLP-1 class, the class comparison report provides head-to-head data on all approved agents.
Lean Mass Loss During Weight Loss
Lean mass loss during weight reduction isn't unique to GLP-1 therapy. It's a fundamental physiological response to caloric deficit that occurs with every weight loss method, from surgery to dieting to exercise. The body, facing an energy shortfall, doesn't exclusively tap into fat reserves. It also breaks down lean tissue for gluconeogenesis, amino acid supply, and energy production. Understanding this baseline physiology is essential before evaluating whether GLP-1 drugs worsen the problem or simply mirror it.
The Quarter Rule and Its Origins
The traditional rule of thumb, sometimes called Forbes' rule, holds that approximately 25% of weight lost through caloric restriction comes from fat-free mass (FFM) and 75% from fat mass. This ratio was established through decades of metabolic ward studies and dietary interventions. Forbes GE documented it in a landmark 2000 paper showing that the FFM fraction depends on initial body fat percentage: leaner individuals lose proportionally more lean mass, while those with higher starting body fat lose proportionally more fat.
That 25% figure, however, comes with major caveats. It represents an average across populations that often didn't perform resistance exercise and consumed suboptimal protein. When you layer on structured training and adequate protein, the lean mass fraction of weight loss can drop to 10-15%. Conversely, very-low-calorie diets without exercise can push the ratio to 35% or higher.
Mechanisms of Lean Tissue Loss in Caloric Deficit
Several interconnected pathways drive muscle loss during energy restriction. The most important is a reduction in muscle protein synthesis (MPS). When caloric intake drops below maintenance, the mTORC1 signaling pathway, which drives MPS, becomes less responsive to both amino acids and mechanical stimulation. Studies using stable isotope tracers show that MPS rates decline by 15-25% within the first week of a caloric deficit, even when protein intake remains constant.
Simultaneously, muscle protein breakdown (MPB) increases. The ubiquitin-proteasome pathway and autophagy-lysosome pathway both upregulate in response to low energy availability. Cortisol levels rise during prolonged caloric restriction, further promoting protein catabolism. The net result is a shift in muscle protein balance from net synthesis (or equilibrium) to net breakdown.
The Role of Insulin and IGF-1
Insulin is powerfully anti-catabolic for skeletal muscle. During caloric restriction, fasting insulin levels drop substantially, removing one of the key brakes on muscle protein breakdown. Insulin-like growth factor 1 (IGF-1), which works downstream of growth hormone to stimulate MPS and satellite cell activation, also decreases during energy deficit. The combination of lower insulin and lower IGF-1 creates a hormonal environment that favors lean tissue loss.
GLP-1 receptor agonists add a layer of complexity here. While they improve insulin sensitivity and beta-cell function (which could theoretically support muscle anabolism), the magnitude of caloric restriction they induce, often 25-40% below maintenance, overwhelms these positive signals. The net hormonal effect remains catabolic for skeletal muscle, at least without deliberate countermeasures. For those interested in supporting growth hormone pathways, CJC-1295/Ipamorelin and sermorelin work through natural GH secretion mechanisms.
The Speed Factor
Rate of weight loss is a critical determinant of body composition outcomes. Faster weight loss consistently produces a higher lean-mass-to-fat-mass loss ratio. A systematic review by Ashtary-Larky D et al. (2020) analyzed 29 studies and found that losing more than 1% of body weight per week increased lean mass losses by approximately 30% compared to slower approaches. The relevance to GLP-1 therapy is immediate: semaglutide 2.4 mg produces weight loss rates of 1-2% of body weight per month during the first 6 months, placing most patients in a moderate-to-fast weight loss trajectory.
Tirzepatide at maximum dose (15 mg) produces even faster weight loss, with some participants in the SURMOUNT trials losing 3-4% of body weight per month during peak efficacy. This speed, while impressive for total weight reduction, creates a larger window for lean mass depletion. Our tirzepatide guide covers the dose-response relationship in detail.
Age and Sex Differences
Older adults face a disproportionate risk of lean mass loss during weight reduction. After age 30, skeletal muscle mass declines at approximately 0.5-1% per year even without deliberate weight loss. This age-related muscle wasting, termed sarcopenia, accelerates after age 60. When caloric restriction is superimposed on this baseline trajectory, the combined effect can be dramatic.
A 2022 study by Villareal DT et al. in adults over 65 found that intentional weight loss of 10% body weight resulted in a 4.8% reduction in lean body mass, with corresponding declines in grip strength and gait speed. For older GLP-1 users, the stakes are higher than for younger patients. The potential loss of physical independence is a real and underappreciated risk.
Sex differences also matter. Men typically lose a greater absolute amount of lean mass than women during weight loss, largely because they start with more. However, women may lose a greater proportion of their starting lean mass relative to total weight lost, particularly postmenopausal women whose declining estrogen levels reduce the anabolic stimulus for muscle. These differences argue for sex-specific protein and training recommendations, which we address in later sections.
What Makes GLP-1-Induced Weight Loss Different
Three features distinguish GLP-1-mediated weight loss from standard caloric restriction in terms of lean mass impact. First, appetite suppression is often so profound that patients struggle to consume adequate protein. When you simply aren't hungry, hitting 1.2-1.6 g/kg/day of protein feels like a chore. Second, the nausea and early satiety associated with GLP-1 drugs can push patients toward low-protein, carbohydrate-heavy comfort foods that provide calories without the amino acid stimulus needed for MPS. Third, the sheer magnitude of weight loss, often 15-25% of body weight, means that even a normal 25% lean mass fraction translates to substantial absolute muscle loss.
There's also a potentially unique pharmacological dimension. GLP-1 receptors are expressed in skeletal muscle, though at low density compared to pancreas and brain. Some in vitro studies have suggested that GLP-1 receptor activation could influence muscle metabolism directly, but the clinical significance of this remains uncertain. Hong Y et al. (2019) showed that GLP-1 treatment of cultured myotubes influenced AMPK signaling, but whether this translates to meaningful muscle effects in humans at therapeutic doses is an open question.
Measuring Body Composition: Methods and Their Limitations
How we measure lean mass matters enormously for interpreting trial data. The gold standard is dual-energy X-ray absorptiometry (DEXA), which provides regional and whole-body estimates of fat mass, lean mass, and bone mineral content. Most GLP-1 clinical trials with body composition substudies used DEXA.
But DEXA has limitations. It measures fat-free mass, not muscle mass specifically. Fat-free mass includes water, glycogen, connective tissue, and organ tissue in addition to skeletal muscle. During the first weeks of any weight loss intervention, glycogen depletion and associated water loss account for a substantial portion of apparent "lean mass" reduction. This means early DEXA measurements likely overestimate true skeletal muscle loss.
Bioelectrical impedance analysis (BIA), used in some real-world studies, is even more susceptible to hydration status artifacts. CT-based measurements of specific muscle cross-sectional areas (like mid-thigh or psoas) provide more direct assessments of actual muscle tissue, but these are rarely included in large trials due to radiation exposure and cost.
The practical implication is that when a trial reports "39% of weight lost was lean mass," the true skeletal muscle component is probably lower, perhaps 25-30%. This is still a meaningful amount, but the distinction matters for clinical counseling. Use the dosing calculator and consult with your provider to understand your individualized risk profile.
The Metabolic Consequences of Lean Mass Loss
Resting metabolic rate (RMR) is strongly correlated with lean body mass. Each kilogram of lean tissue contributes approximately 13-15 kcal/day to RMR. Lose 5 kg of lean mass and your daily energy expenditure drops by 65-75 calories. Over a year, that adds up to roughly 7-8 pounds of potential weight regain if caloric intake isn't adjusted downward to match.
This creates the metabolic adaptation trap that makes weight maintenance so difficult after GLP-1 discontinuation. Patients who lose significant lean mass have a lower metabolic rate than their new body weight would predict, a phenomenon called adaptive thermogenesis or metabolic adaptation. Their bodies are essentially "undersized" relative to their metabolic capacity, creating persistent drive toward weight regain. The lifestyle hub addresses long-term weight maintenance strategies in detail.
Beyond metabolic rate, lean mass loss impairs glucose disposal. Skeletal muscle is responsible for approximately 80% of insulin-stimulated glucose uptake. Reducing muscle mass directly reduces the body's capacity to clear glucose from the bloodstream, potentially undermining one of the primary therapeutic goals of GLP-1 therapy in patients with type 2 diabetes. This paradox, where a diabetes drug might worsen glucose disposal capacity through muscle loss, underscores the importance of muscle preservation strategies.
Body Composition Data from GLP-1 Trials
Quantifying lean mass changes on GLP-1 drugs requires examining the body composition substudies embedded within large phase 3 trials. These substudies typically use DEXA to measure fat mass, lean mass, and bone mineral density at baseline and study endpoint. The data, while not always the primary focus of the trials, provides the clearest picture of what happens to body composition during pharmacological weight loss.
STEP 1: Semaglutide 2.4 mg Body Composition
The STEP 1 trial enrolled 1,961 adults with obesity or overweight plus at least one weight-related comorbidity. A DEXA substudy of 140 participants provided the most detailed body composition data for semaglutide 2.4 mg. Over 68 weeks, the semaglutide group lost an average of 15.3 kg of total body weight. Of this, approximately 6.0 kg (39.2%) was lean mass and 8.4 kg (54.9%) was fat mass, with the remainder being bone mineral and water content.
That 39% lean mass fraction attracted significant attention and concern. It's higher than the classic 25% benchmark, though several factors complicate direct comparison. The rate of weight loss in STEP 1 was faster than typical dietary interventions, the participants were not prescribed structured exercise, and protein intake was not specifically targeted or monitored. All of these factors skew the lean mass ratio upward.
Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183.
STEP 3: Semaglutide with Intensive Behavioral Therapy
STEP 3 combined semaglutide 2.4 mg with intensive behavioral therapy (IBT), including recommendations for increased physical activity and caloric restriction. The body composition substudy showed a modestly improved lean mass preservation compared to STEP 1, with lean mass accounting for approximately 32-35% of total weight lost. This difference, while not enormous, suggests that structured behavioral support, which likely led to more physical activity and somewhat better dietary choices, can shift body composition outcomes even without a formal resistance training protocol.
SURMOUNT Trials: Tirzepatide Body Composition
Tirzepatide, the dual GIP/GLP-1 receptor agonist, produced even greater total weight loss than semaglutide in clinical trials. The SURMOUNT-1 trial showed mean weight reductions of 15.0%, 19.5%, and 20.9% at the 5 mg, 10 mg, and 15 mg doses, respectively. A DEXA substudy of approximately 200 participants provided body composition data.
The lean mass fraction of total weight lost with tirzepatide ranged from 29-33% across doses, which is actually slightly more favorable than the semaglutide STEP 1 data. Several hypotheses explain this difference. GIP receptor activation may have muscle-protective properties that partially offset the catabolic effects of energy restriction. GIP receptors are expressed in skeletal muscle, and in vitro data suggests GIP may influence lipid metabolism within myocytes. Alternatively, the difference could reflect methodological variations between the substudies.
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. New England Journal of Medicine. 2022;387(3):205-216. DOI: 10.1056/NEJMoa2206038.
Lean Mass as Percentage of Total Weight Lost by Intervention
Data synthesized from STEP 1, SURMOUNT-1, and Lundgren et al. (2024). "Semaglutide + RT" refers to GLP-1 therapy combined with structured resistance training.
SCALE Trials: Liraglutide Body Composition
Liraglutide 3.0 mg (Saxenda), the earlier daily GLP-1 agonist, produced more modest weight loss than semaglutide or tirzepatide but still showed meaningful lean mass changes. In the SCALE Obesity and Prediabetes trial, participants lost a mean of 8.4 kg, with lean mass representing approximately 28% of total weight lost. The lower lean mass fraction likely reflects the slower rate and smaller magnitude of weight loss compared to semaglutide.
Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. New England Journal of Medicine. 2015;373(1):11-22. DOI: 10.1056/NEJMoa1411892.
Head-to-Head Comparison Table
| Drug | Trial | Total Weight Lost (kg) | Lean Mass Lost (kg) | Lean Mass % of Total | Duration |
|---|---|---|---|---|---|
| Semaglutide 2.4 mg | STEP 1 | 15.3 | 6.0 | 39% | 68 wk |
| Semaglutide 2.4 mg + IBT | STEP 3 | 16.8 | 5.5 | ~33% | 68 wk |
| Tirzepatide 5 mg | SURMOUNT-1 | 14.1 | 4.2 | ~30% | 72 wk |
| Tirzepatide 10 mg | SURMOUNT-1 | 18.6 | 5.6 | ~30% | 72 wk |
| Tirzepatide 15 mg | SURMOUNT-1 | 20.1 | 6.6 | ~33% | 72 wk |
| Liraglutide 3.0 mg | SCALE | 8.4 | 2.4 | ~28% | 56 wk |
| Diet alone (reference) | Multiple | Variable | Variable | ~25% | Variable |
| GLP-1 + Resistance Training | Lundgren et al. | Similar | Reduced | ~16-18% | Variable |
The STEP 1 Extension: What Happens After Discontinuation
Perhaps the most concerning body composition data comes from the STEP 1 extension study, which followed participants for 1 year after semaglutide discontinuation. Participants regained approximately two-thirds of their lost weight over 52 weeks. But the composition of regained weight appeared to favor fat over lean tissue. While the DEXA substudy during the extension was limited, the available data suggested that patients ended up with a higher fat-to-lean mass ratio than they had before starting treatment.
This "worse than baseline" body composition outcome has profound implications. It means that a cycle of GLP-1-induced weight loss followed by drug discontinuation and weight regain could progressively worsen body composition over time, essentially the same "yo-yo dieting" concern that has plagued dieters for decades, but with pharmacological acceleration.
Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide. Diabetes, Obesity and Metabolism. 2022;24(8):1553-1564. DOI: 10.1111/dom.14725.
Retatrutide and Next-Generation Agents
Retatrutide, the triple GIP/GLP-1/glucagon receptor agonist, produced weight losses exceeding 24% in phase 2 trials. Body composition data from these early trials is limited but suggests a lean mass fraction of approximately 30-35%. The glucagon receptor component of retatrutide may influence lean mass outcomes differently than pure GLP-1 agonists, as glucagon has complex effects on both hepatic glucose production and amino acid metabolism. The retatrutide guide tracks the evolving data.
Cagrilintide/semaglutide (CagriSema) also shows high-magnitude weight loss with body composition profiles broadly similar to semaglutide alone, based on early trial data. The amylin component may have some muscle-protective properties through its effects on nutrient partitioning, but this remains speculative. For the latest on this combination, see our CagriSema guide.
What the Data Tells Us
Three patterns emerge from the aggregate body composition data. First, all GLP-1 agonists produce lean mass loss that exceeds the traditional 25% benchmark when no structured exercise is prescribed. Second, the magnitude of lean mass loss scales roughly with total weight lost and speed of weight loss, meaning higher doses and more aggressive titration schedules tend to produce worse lean mass outcomes. Third, the addition of any form of structured physical activity, and especially resistance training, substantially improves the ratio.
The clinical implication is straightforward: prescribing a GLP-1 drug without addressing muscle preservation is only doing half the job. Every prescription should come with a muscle protection plan. For those exploring GLP-1 weight loss options, understanding these body composition dynamics is essential for long-term success.
Protein Requirements on GLP-1 Therapy
Protein intake is the single most controllable variable for muscle preservation during GLP-1-mediated weight loss. While resistance training provides the mechanical stimulus for muscle retention, protein supplies the raw materials. Without adequate amino acid availability, no amount of training can fully prevent lean tissue loss. The challenge on GLP-1 drugs is that the very appetite suppression that makes them effective for weight loss also makes hitting protein targets genuinely difficult.
How Much Protein Do You Need?
The standard Recommended Dietary Allowance (RDA) for protein is 0.8 g/kg/day, but this target was established for sedentary individuals maintaining weight, not for people actively losing weight on powerful appetite-suppressing drugs. Current evidence supports substantially higher intakes for muscle preservation during caloric restriction.
The International Society of Sports Nutrition (ISSN), the American College of Sports Medicine (ACSM), and multiple systematic reviews converge on a range of 1.2-1.6 g/kg/day for muscle preservation during weight loss. Some researchers advocate even higher, with Helms ER et al. (2014) recommending 2.3-3.1 g/kg of fat-free mass per day for lean athletes in caloric deficit. For most GLP-1 patients, who are not competitive athletes, 1.2-1.6 g/kg of total body weight provides a practical and evidence-based target.
What This Looks Like in Practice
| Body Weight | Protein at 1.2 g/kg | Protein at 1.6 g/kg | Per Meal (4 meals) |
|---|---|---|---|
| 150 lb (68 kg) | 82 g/day | 109 g/day | 20-27 g |
| 180 lb (82 kg) | 98 g/day | 131 g/day | 25-33 g |
| 200 lb (91 kg) | 109 g/day | 145 g/day | 27-36 g |
| 220 lb (100 kg) | 120 g/day | 160 g/day | 30-40 g |
| 250 lb (114 kg) | 136 g/day | 182 g/day | 34-46 g |
The Leucine Threshold
Not all protein is created equal for muscle protein synthesis. The branched-chain amino acid leucine acts as a molecular trigger for the mTORC1 pathway, which initiates MPS. Research by Layman DK and others has established that approximately 2.5-3.0 grams of leucine per meal is needed to maximally stimulate MPS. This is sometimes called the "leucine threshold."
Different protein sources contain different amounts of leucine. Whey protein is the richest source at approximately 11% leucine by weight, meaning 25-30 grams of whey provides the threshold dose. Eggs contain about 8.5% leucine, chicken breast about 7.5%, and most plant proteins fall in the 6-7% range. For GLP-1 patients struggling with appetite, whey protein shakes offer the most leucine per unit of food volume, making them an ideal choice when solid food feels unappealing.
Protein Timing and Distribution
Spreading protein intake across the day rather than concentrating it in one or two meals produces better muscle outcomes. The "muscle-full" concept described by Atherton PJ and colleagues suggests that MPS reaches a ceiling after approximately 0.4 g/kg of protein per meal, beyond which additional protein at that sitting provides diminishing returns. The stimulus then resets, and the next meal can trigger another MPS response.
For a 180-pound person targeting 130 grams of protein daily, the optimal distribution would be roughly 30-35 grams across 4 eating occasions. This is where GLP-1 patients often struggle. Many find they can only eat two meals per day due to profound appetite suppression, and those meals are often small. The result is protein intake clustering around 40-60 grams per day, less than half of the recommended amount.
Practical Strategies for Hitting Protein Targets on GLP-1 Drugs
Strategy 1: Protein-First Eating
Start every meal with the protein component before touching carbohydrates or fats. When satiety kicks in early, at least you've consumed the most important macronutrient. A 4-ounce chicken breast (35 g protein) eaten before a side salad and rice ensures the protein is in even if you can't finish the rest.
Strategy 2: Liquid Protein Sources
When solid food feels impossible, liquid calories are easier to consume. A 40-gram whey protein shake in 8 ounces of water can be sipped over 30 minutes and provides more than a meal's worth of high-quality protein. Greek yogurt smoothies, bone broth, and protein-fortified milk are other options that go down easily when appetite is minimal.
Strategy 3: Protein-Dense Snacking
Keep protein-dense snacks accessible: beef jerky (9-10 g per ounce), string cheese (7 g per stick), hard-boiled eggs (6 g each), and Greek yogurt (15-20 g per serving). Even on days when meals are small, two or three protein snacks can add 30-40 grams to the daily total.
Strategy 4: Protein Supplementation
For patients consistently falling short of protein targets despite best efforts, supplementation becomes necessary rather than optional. Whey protein isolate is the most studied and efficient option. Casein provides slower-digesting protein suitable for evening consumption. Plant-based blends (pea + rice protein) offer an alternative for dairy-intolerant patients. Essential amino acid (EAA) supplements, taken between meals, can provide an MPS stimulus with minimal caloric load and no GI distress.
Protein Quality and Digestibility
The Digestible Indispensable Amino Acid Score (DIAAS) ranks protein sources by their amino acid profile and digestibility. Whey protein isolate scores highest at approximately 1.09, followed by whole eggs (1.13), milk (1.14), and chicken breast (1.08). Most plant proteins score lower: soy at 0.90, pea protein at 0.82, and wheat protein at 0.40. For GLP-1 patients eating reduced quantities, choosing high-DIAAS protein sources maximizes the muscle-protective benefit per gram consumed.
CLINICAL PEARL
Many GLP-1 patients report that their protein intake drops to 40-60 g/day during the first 2-3 months of therapy. Proactive protein counseling at the time of drug initiation, not after muscle loss has occurred, is critical. Consider referring patients to a registered dietitian experienced with GLP-1 therapy for individualized meal planning.
What Happens When Protein Is Inadequate
A study by Pasiakos SM et al. (2013) directly tested the impact of protein dose on lean mass during caloric restriction in young, healthy adults. Participants consuming the RDA (0.8 g/kg/day) lost significantly more lean mass than those consuming 1.6 g/kg/day, even though total weight loss was similar. The high-protein group lost 1.5 kg of lean mass versus 3.2 kg in the standard-protein group over a 21-day deficit period. Double the protein, half the muscle loss.
Pasiakos SM, Cao JJ, Margolis LM, et al. Effects of high-protein diets on fat-free mass and muscle protein synthesis following weight loss. FASEB Journal. 2013;27(9):3837-3847. DOI: 10.1096/fj.13-230227.
For those who want to explore peptide-based approaches to supporting protein metabolism and muscle anabolism, IGF-1 LR3 works directly on muscle tissue to promote protein synthesis. Similarly, MK-677 (Ibutamoren) supports growth hormone release, which has downstream effects on IGF-1 levels and nitrogen balance. Both should only be considered under clinical supervision.
Resistance Training Protocols
Resistance training is the most powerful single intervention for preserving lean mass during GLP-1-mediated weight loss. It works by providing a mechanical stimulus that signals skeletal muscle to maintain its mass even in the face of caloric deficit. The evidence for this is strong, consistent, and dose-responsive: more resistance training equals less muscle loss, down to a floor of roughly 10-15% of total weight lost as lean mass under optimal conditions.
The Landmark Lundgren Study
The most directly relevant study was published by Lundgren JR, Janus C, Jensen SBK, et al. in 2024. This randomized controlled trial assigned adults on liraglutide therapy to either a supervised resistance training program or usual care. Both groups received liraglutide 3.0 mg daily and dietary counseling. The resistance training group performed 3 sessions per week of progressive resistance exercises targeting all major muscle groups.
Results were striking. Total weight loss was similar between groups (approximately 12-13% of body weight), but body composition differed dramatically. In the usual care group, lean mass accounted for about 35% of weight lost. In the resistance training group, that number dropped to just 16%. The training group also showed preserved or improved physical function measures, including grip strength and chair-rise speed, while the usual care group showed functional declines.
Lundgren JR, Janus C, Jensen SBK, et al. Healthy weight loss maintenance with exercise, liraglutide, or both combined. New England Journal of Medicine. 2024;391(11):1020-1031. DOI: 10.1056/NEJMoa2312892.
Recommended Training Protocol: The Essentials
Based on the available evidence, here is a resistance training protocol specifically designed for GLP-1 patients focused on muscle preservation. This isn't a bodybuilding program; it's a muscle-protective prescription.
Frequency
Train 3 days per week minimum, with at least 48 hours between sessions targeting the same muscle groups. A Monday-Wednesday-Friday schedule works well for most people. If you can manage 4 sessions per week, an upper-lower split (upper body Monday/Thursday, lower body Tuesday/Friday) provides additional volume without excessive fatigue.
Exercise Selection
Prioritize compound movements that engage multiple joints and large muscle groups. These exercises provide the greatest anabolic stimulus per unit of training time:
- Lower body: Barbell or goblet squats, Romanian deadlifts, leg press, lunges, hip thrusts
- Upper body push: Bench press (barbell or dumbbell), overhead press, push-ups (weighted if possible)
- Upper body pull: Barbell or dumbbell rows, lat pulldowns, chin-ups or assisted chin-ups
- Core: Planks, pallof press, loaded carries (farmer's walks)
Volume and Intensity
Perform 3-4 sets of 6-12 repetitions per exercise, with loads that bring you within 2-3 repetitions of failure. Research by Schoenfeld BJ et al. (2017) demonstrates that the proximity to muscular failure is the critical driver of hypertrophic stimulus, not the specific rep range. For GLP-1 patients who may be training on reduced caloric intake, staying 2-3 reps from failure (rather than training to absolute failure) helps manage recovery demands.
Progressive Overload
The training must be progressive to remain effective. This means gradually increasing load, volume, or both over time. A simple approach: when you can complete all prescribed sets and reps with good form, increase the weight by 2.5-5 pounds at the next session. Even small, consistent increases in load provide the signal that muscle tissue is needed and should be preserved.
Sample 3-Day Full-Body Program
| Day | Exercise | Sets x Reps | Rest |
|---|---|---|---|
| Day A (Mon) | Barbell Back Squat | 3 x 8-10 | 2-3 min |
| Dumbbell Bench Press | 3 x 8-12 | 2 min | |
| Barbell Row | 3 x 8-10 | 2 min | |
| Overhead Press | 3 x 8-12 | 2 min | |
| Plank | 3 x 30-60s | 1 min | |
| Day B (Wed) | Romanian Deadlift | 3 x 8-10 | 2-3 min |
| Incline Dumbbell Press | 3 x 10-12 | 2 min | |
| Lat Pulldown | 3 x 10-12 | 2 min | |
| Leg Press | 3 x 10-12 | 2 min | |
| Farmer's Walk | 3 x 40 yards | 1 min | |
| Day C (Fri) | Goblet Squat | 3 x 10-12 | 2 min |
| Push-ups (weighted) | 3 x max | 2 min | |
| Cable Row | 3 x 10-12 | 2 min | |
| Walking Lunges | 3 x 10/leg | 2 min | |
| Pallof Press | 3 x 12/side | 1 min |
Adapting for Low Energy Availability
GLP-1 patients often report lower energy levels during training sessions, especially in the first months of therapy. This is expected when caloric intake drops significantly. The key adaptation is to reduce total training volume by 20-30% compared to a maintenance or bulking program, while keeping intensity (load relative to maximum) as high as possible.
Think of it this way: volume can be sacrificed to some degree, but intensity cannot. Three hard sets of squats at 80% of your max will preserve more muscle than six easy sets at 50%. The mechanical tension signal is what matters for muscle retention, and that signal comes from heavy loads, not from high rep counts with light weights.
For Beginners or Those Returning to Training
If you haven't trained with weights before, or if it's been years, don't jump into a heavy barbell program. Start with machines and bodyweight exercises for the first 4-6 weeks to establish movement patterns and build base-level strength. A leg press is easier to learn than a barbell squat, and a chest press machine is safer than a bench press for novices. The muscle-preserving stimulus from machines is equivalent to free weights; the muscles don't know what's providing the resistance.
Progress to free weights as competence and confidence grow. Consider working with a qualified personal trainer for at least the initial sessions to establish proper form. The investment in instruction pays dividends in injury prevention and training effectiveness. The lifestyle hub has additional resources on exercise programming.
Cardio: Helpful or Harmful?
Cardiovascular exercise is often the default recommendation for weight loss, but its role alongside GLP-1 therapy requires careful consideration. Moderate cardio (walking, cycling, swimming at conversational intensity) supports cardiovascular health, mental well-being, and recovery between resistance sessions. It should be included.
However, excessive cardio, particularly high-volume endurance training, can interfere with muscle preservation. The "interference effect" described by Hickson RC (1980) shows that concurrent heavy endurance and resistance training compromises muscle adaptation to the resistance work. For GLP-1 patients, a practical guideline is to prioritize resistance training and limit cardio to 2-3 sessions of moderate-intensity work (30-45 minutes) per week. Walking is ideal because it provides health benefits without significant interference with muscle recovery.
Recovery Considerations
Recovery capacity is reduced during caloric deficit. Sleep becomes even more important than usual, with 7-9 hours being the target range. Poor sleep increases cortisol, reduces growth hormone secretion, and impairs muscle protein synthesis. For patients interested in supporting sleep quality and natural GH release, DSIP (Delta Sleep-Inducing Peptide) may be worth discussing with a provider.
Stress management also influences muscle preservation. Chronically elevated cortisol is directly catabolic for skeletal muscle, and the psychological stress of significant dietary restriction can compound this effect. Mindfulness practices, adequate social support, and realistic expectations about the pace of body composition improvement all contribute to better outcomes.
Creatine & Supplement Strategies

Beyond protein and resistance training, several supplements have meaningful evidence for supporting muscle preservation during caloric deficit. The evidence base varies substantially, so we'll tier the recommendations from strongest to weakest scientific support. Creatine monohydrate stands in a class by itself, while other compounds have promising but less complete data.
Tier 1: Creatine Monohydrate
Creatine monohydrate is the single most studied and effective supplement for muscle performance and lean mass support. Over 500 peer-reviewed studies support its benefits. During caloric restriction, creatine serves multiple functions: it replenishes phosphocreatine stores for high-intensity exercise performance, increases intramuscular water content (which may support cellular signaling for muscle maintenance), and appears to enhance the muscle-protein-synthetic response to resistance training.
A meta-analysis by Chilibeck PD et al. (2017) found that creatine supplementation during resistance training programs increased lean mass by an average of 1.4 kg more than resistance training alone. During caloric restriction, this effect translates to better lean mass preservation rather than net muscle gain.
Dosing Protocol
- Maintenance dose: 3-5 grams daily (no loading phase required, though loading with 20 g/day for 5-7 days saturates stores faster)
- Timing: Any time of day; consistency matters more than timing
- Form: Creatine monohydrate is the gold standard. No other form (HCl, ethyl ester, buffered) has shown superior bioavailability or efficacy
- Duration: Continuous use throughout GLP-1 therapy and beyond
CREATINE SAFETY NOTE
Creatine monohydrate has an excellent safety profile across decades of research. It does not damage kidneys in healthy individuals. It may increase serum creatinine levels slightly, which can be mistaken for kidney dysfunction on routine labs. Alert your healthcare provider that you're taking creatine so they can interpret lab results appropriately. Adequate hydration (8+ glasses of water daily) is recommended.
Tier 2: Vitamin D
Vitamin D deficiency is common in adults with obesity, with prevalence rates of 40-60% depending on the population studied. Vitamin D receptors are expressed in skeletal muscle, and deficiency is associated with reduced muscle strength, impaired MPS, and increased risk of falls. Several studies have shown that correcting vitamin D deficiency to optimal levels (40-60 ng/mL) improves muscle function, particularly in older adults.
For GLP-1 patients, ensure serum 25-hydroxyvitamin D is at least 30 ng/mL, with many experts targeting 40-60 ng/mL. Most adults with obesity require 2,000-5,000 IU of vitamin D3 daily to achieve these levels. Get a baseline blood test and recheck after 3 months of supplementation.
Tier 2: Omega-3 Fatty Acids
EPA and DHA, the long-chain omega-3 fatty acids found in fish oil, have shown muscle-protective properties in several studies. Smith GI et al. (2011) demonstrated that omega-3 supplementation enhanced the MPS response to amino acid infusion in older adults. The mechanism appears to involve incorporation of EPA and DHA into muscle cell membranes, improving the sensitivity of the mTORC1 signaling pathway to anabolic stimuli.
A dose of 2-4 grams of combined EPA/DHA daily is commonly recommended. Look for products that provide at least 1 gram of EPA, as EPA appears to be the more muscle-relevant omega-3.
Tier 3: HMB (Beta-Hydroxy Beta-Methylbutyrate)
HMB is a metabolite of leucine that has shown anti-catabolic properties in some studies, particularly in older adults and clinical populations. A meta-analysis by Wu H et al. (2015) found that HMB supplementation (3 grams/day) preserved lean mass during bed rest and caloric restriction in elderly subjects. The evidence in younger, healthy adults is less convincing, and many sports nutrition researchers consider the effect size small relative to resistance training and protein optimization.
For GLP-1 patients over 60 or those unable to perform resistance training, HMB at 3 grams/day may provide modest additional lean mass protection. For younger, active patients, the benefit over adequate protein and creatine is likely marginal.
Peptide-Based Growth Hormone Secretagogues
Growth hormone (GH) is a potent anabolic and lipolytic hormone that declines with age and caloric restriction. Several peptides support the body's natural GH production through different mechanisms, and some clinicians incorporate these into muscle-preservation protocols alongside GLP-1 therapy.
CJC-1295/Ipamorelin
CJC-1295/Ipamorelin is one of the most commonly used GH secretagogue combinations. CJC-1295 is a growth hormone-releasing hormone (GHRH) analog that extends the half-life of the natural GH pulse, while Ipamorelin is a selective ghrelin mimetic that stimulates GH release without significantly raising cortisol or prolactin. Together, they produce a sustained elevation in GH and IGF-1 levels that supports nitrogen balance, protein synthesis, and lean tissue preservation.
Clinical use typically involves subcutaneous injections administered before bedtime to capitalize on the natural nocturnal GH surge. Patients report improved sleep quality, enhanced recovery from training, and better body composition outcomes when added to their GLP-1 protocol. Our peptide research hub covers GH secretagogues in depth.
MK-677 (Ibutamoren)
MK-677 is an oral growth hormone secretagogue that works through the ghrelin receptor to stimulate GH release. Its primary advantage is oral bioavailability, eliminating the need for injections. Studies by Nass R et al. (2008) showed that MK-677 increased IGF-1 levels to those of healthy young adults in elderly subjects, along with improvements in lean body mass.
A potential concern with MK-677 in the context of GLP-1 therapy is its appetite-stimulating effect. Since appetite suppression is a key mechanism of GLP-1 drugs, adding an appetite-enhancing compound may partially counteract the weight loss benefits. However, some clinicians view this as an advantage, arguing that the appetite boost from MK-677 specifically helps patients consume adequate protein rather than simply eating more of everything. This remains an area requiring careful clinical judgment.
BPC-157 and TB-500 for Recovery
While not directly anabolic for muscle, BPC-157 and TB-500 support tissue repair and recovery processes that indirectly benefit muscle preservation. BPC-157 has demonstrated wound healing, anti-inflammatory, and tendon/ligament repair properties in preclinical studies. TB-500 promotes angiogenesis and tissue remodeling. For GLP-1 patients engaged in resistance training, these peptides may support recovery from training-induced tissue stress, reducing injury risk and allowing more consistent training adherence.
The BPC-157/TB-500 blend offers both compounds in a single preparation for convenience. Our BPC-157 guide covers the research base in detail.
Supplements to Avoid or Approach with Caution
Several popular supplements lack meaningful evidence for muscle preservation during weight loss. Branched-chain amino acids (BCAAs) in isolation are unnecessary if total protein intake is adequate, as whole protein sources already contain BCAAs in optimal ratios. Testosterone boosters marketed as "natural" typically contain herbal extracts (tribulus, fenugreek, ashwagandha) with minimal evidence for clinically meaningful testosterone elevation. CLA (conjugated linoleic acid) showed early promise for body composition but subsequent meta-analyses revealed effects too small to be clinically relevant.
The supplement stack should be simple: creatine monohydrate, vitamin D (if deficient), omega-3s, and high-quality protein. Everything beyond that is gravy, with diminishing returns on investment.
'Ozempic Face' and Skin Changes
"Ozempic face" entered the popular lexicon in 2023, describing the gaunt, hollow, prematurely aged facial appearance that some patients develop after significant weight loss on GLP-1 drugs. It's not a medical diagnosis but rather a colloquial term that captures a real cosmetic concern. Understanding what causes it, and how it differs from systemic muscle loss, helps patients set realistic expectations and take preventive action.
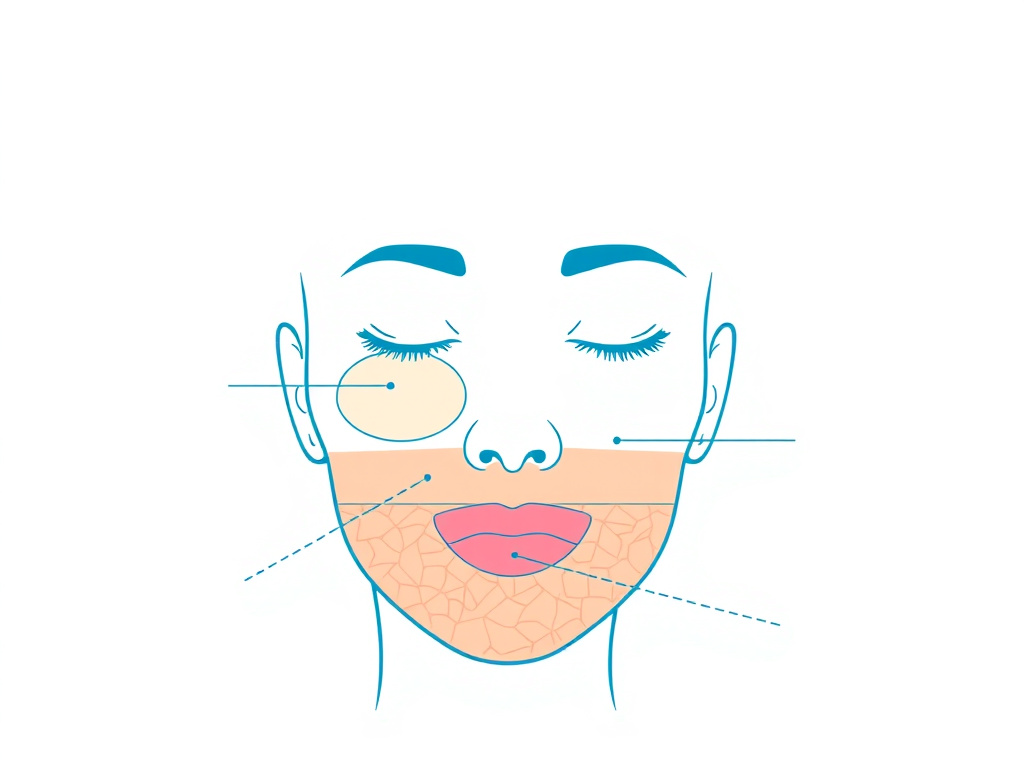
What's Actually Happening to the Face
The face contains relatively little skeletal muscle. Facial changes during weight loss are driven almost entirely by subcutaneous fat loss rather than muscle wasting. The face has several distinct fat compartments, including the malar fat pad (cheekbone area), buccal fat pad (mid-face), nasolabial fat pad, and periorbital fat. These compartments provide the youthful volume and contour that we associate with a healthy facial appearance.
When significant weight loss occurs, these facial fat pads shrink. The overlying skin, which may have reduced elasticity due to age, sun damage, or smoking, cannot fully contract to match the reduced volume. The result is sagging skin, deepened nasolabial folds, hollowed cheeks, and a generally gaunt appearance. This process happens with any weight loss method, but the speed and magnitude of GLP-1-induced weight loss can make it more noticeable and more distressing to patients.
Risk Factors for Facial Volume Loss
- Age over 40: Skin elasticity declines progressively, reducing the capacity to "bounce back" after volume loss
- Total weight loss exceeding 15%: Greater magnitude of weight loss increases facial fat depletion
- Speed of weight loss: Rapid loss gives skin less time to adapt
- Smoking history: Tobacco damages collagen and elastin, worsening skin laxity
- Sun damage: UV exposure degrades dermal collagen
- Genetics: Some individuals naturally have less facial fat or thinner skin
- Low protein intake: Inadequate amino acids impair collagen synthesis and skin renewal
Prevention Strategies
Optimize Protein and Collagen Intake
Adequate protein supports collagen synthesis in the dermis. Some clinicians recommend supplemental collagen peptides (10-15 g/day) to provide the specific amino acids (glycine, proline, hydroxyproline) needed for collagen production. A study by Proksch E et al. (2014) showed that oral collagen supplementation improved skin elasticity after 8 weeks. While this won't prevent facial fat loss, it may support skin quality during the transition.
Sun Protection
UV radiation is the primary driver of extrinsic skin aging. Daily broad-spectrum SPF 30+ sunscreen, combined with UV-protective clothing and limited sun exposure, preserves dermal collagen and elastin. This is basic but often overlooked during weight loss programs.
Topical Interventions
Retinoids (tretinoin 0.025-0.1%) increase collagen production and skin cell turnover, improving skin quality over 3-6 months of consistent use. GHK-Cu is a copper peptide that has demonstrated collagen-stimulating, anti-inflammatory, and wound-healing properties in skin studies. GHK-Cu topical formulations can be applied directly to facial skin to support dermal remodeling during weight loss.
Consider a Slower Weight Loss Trajectory
If facial appearance is a high priority, discussing a slower dose titration with your provider may be worthwhile. Losing weight at 0.5-0.75% of body weight per week rather than 1-1.5% gives skin more time to adapt. This trade-off between speed of weight loss and cosmetic outcome is a legitimate clinical conversation. For detailed dosing guidance, the dosing calculator can help map out different titration timelines.
Treatment Options If Facial Volume Loss Has Already Occurred
For patients who have already developed noticeable facial volume loss, several interventions can restore a more youthful appearance. These are cosmetic procedures that should be discussed with a qualified dermatologist or plastic surgeon:
- Hyaluronic acid fillers: Products like Juvederm, Restylane, and Sculptra can replace lost volume in specific facial compartments. Results are immediate but temporary (6-18 months depending on the product).
- Fat transfer: Autologous fat grafting removes fat from another body area and injects it into the face. Results are more natural and longer-lasting than synthetic fillers.
- Radiofrequency and ultrasound treatments: Non-invasive skin tightening procedures (Ultherapy, Thermage) stimulate collagen production and provide modest lifting effects.
Distinguishing 'Ozempic Face' from Sarcopenia
It's important to recognize that "Ozempic face" is a cosmetic issue driven by facial fat loss, not a sign of dangerous muscle wasting. A patient can have significant facial volume loss while maintaining excellent lean body mass if they're following a resistance training and protein protocol. Conversely, a patient with a full face can still be losing dangerous amounts of muscle mass if they're sedentary and under-eating protein.
The real dangers of GLP-1-induced body composition change - reduced metabolic rate, impaired glucose disposal, increased fracture risk, functional decline - are related to skeletal muscle and bone loss, not facial fat loss. Keep the priorities straight: protect the muscle first, address cosmetic concerns second. For those exploring comprehensive approaches, NAD+ supplementation supports cellular energy and repair processes that benefit both muscle and skin health. And our science and research page tracks the latest published data on body composition outcomes.
Combination Approaches: GLP-1 + Myostatin Inhibitors
The pharmaceutical industry has recognized that the lean mass problem with GLP-1 drugs is both a clinical concern and a commercial opportunity. Several companies are now developing combination strategies that pair GLP-1-mediated weight loss with agents specifically designed to build or preserve muscle. The most advanced of these target the myostatin/activin pathway, one of the body's primary brakes on muscle growth.
Understanding Myostatin
Myostatin (also called GDF-8) is a member of the TGF-beta superfamily that acts as a negative regulator of skeletal muscle mass. Discovered in 1997 by McPherron AC, Lawler AM, and Lee SJ at Johns Hopkins, myostatin essentially tells muscle tissue to stop growing. Animals with naturally occurring myostatin mutations, like Belgian Blue cattle and certain dog breeds, develop extraordinary musculature.
In humans, myostatin levels increase during caloric restriction and weight loss, further promoting muscle catabolism when it's least wanted. Blocking myostatin or its receptors allows muscle to escape this growth brake, potentially enabling muscle maintenance or even growth during caloric deficit.
Bimagrumab: The Most Advanced Candidate
Bimagrumab is a monoclonal antibody that blocks the activin type II receptor (ActRII), which is the receptor through which myostatin and related ligands (activin A, GDF-11) signal. By blocking this receptor, bimagrumab removes the growth brake on muscle tissue.
A Phase 2 trial by Heymsfield SB, Coleman LA, Miller R, et al. (2021) tested bimagrumab in adults with obesity and type 2 diabetes. The results were remarkable: participants receiving bimagrumab lost 20.5% of their fat mass while simultaneously gaining 3.6% of their lean mass over 48 weeks. This combination of fat loss and muscle gain is virtually unprecedented in any pharmacological weight loss study.
Heymsfield SB, Coleman LA, Miller R, et al. Effect of bimagrumab vs placebo on body fat mass among adults with type 2 diabetes and obesity. JAMA Network Open. 2021;4(1):e2033457. DOI: 10.1001/jamanetworkopen.2020.33457.
Versanis Bio (now acquired by Eli Lilly for $1.93 billion) is developing bimagrumab in combination with semaglutide. Phase 2 data for this combination is expected in 2025-2026 and represents perhaps the most eagerly anticipated body composition study in the GLP-1 space. If bimagrumab can preserve or increase muscle mass while semaglutide drives fat loss, the combination would address the primary limitation of current GLP-1 therapy.
Taldefgrobep: Anti-Myostatin Adnectin
Taldefgrobep alfa is an anti-myostatin adnectin (a small protein scaffold that binds and neutralizes myostatin) being developed by BMS for muscle wasting conditions. While its initial focus is on spinal muscular atrophy, the mechanism is directly relevant to GLP-1-associated lean mass loss. Trials in obesity populations have not yet been announced, but the logic for combination with GLP-1 drugs is compelling.
Activin Receptor Ligand Traps
Several companies are developing activin receptor ligand traps that neutralize not just myostatin but the entire family of related TGF-beta ligands that suppress muscle growth. These broader-acting agents may provide more substantial muscle effects than myostatin-specific inhibitors, as activin A and GDF-11 also contribute to muscle growth limitation.
GLP-1 + Testosterone
Testosterone replacement therapy (TRT) is already used in men with documented hypogonadism and has well-established muscle-building effects. A number of clinicians prescribe testosterone alongside GLP-1 therapy for hypogonadal men, reasoning that normalizing testosterone levels supports muscle preservation during weight loss. The emerging class of oral SARMs (selective androgen receptor modulators) may eventually provide a more targeted option, though none are currently approved for this indication.
For women, the hormonal picture is more complex. Estrogen has muscle-protective properties, and postmenopausal women on GLP-1 therapy may benefit from hormone replacement therapy (HRT) for multiple reasons, including lean mass preservation. This decision requires careful risk-benefit analysis with an endocrinologist.
The Growth Hormone Approach
Growth hormone (GH) is powerfully anabolic for muscle and lipolytic for fat, making it theoretically ideal as a GLP-1 companion. However, synthetic GH therapy (somatropin) is expensive, requires daily injections, and carries risks including fluid retention, joint pain, insulin resistance, and potential cancer concerns with long-term use.
GH secretagogues offer a more measured approach. Rather than providing supraphysiological GH doses, compounds like CJC-1295/Ipamorelin, MK-677, sermorelin, and tesamorelin stimulate the pituitary to release more of its own GH. This preserves the natural pulsatile secretion pattern and negative feedback loops, resulting in a more physiological elevation that's less likely to cause adverse effects.
Tesamorelin, a GHRH analog, is particularly interesting because it's FDA-approved for reducing visceral adipose tissue in HIV-associated lipodystrophy. Its dual effects of reducing visceral fat and supporting lean mass make it a logical candidate for combination with GLP-1 therapy, though this specific combination hasn't been studied in a controlled trial.
MOTS-c and Mitochondrial Peptides
MOTS-c is a mitochondrial-derived peptide that enhances cellular metabolism and exercise capacity. In animal models, MOTS-c treatment improved exercise performance and metabolic health in aged mice. While human data is limited, the peptide's mechanism of action - improving mitochondrial function in skeletal muscle - is relevant to preserving muscle quality during weight loss. The biohacking hub covers emerging mitochondrial peptides.
The Future Landscape
The convergence of anti-obesity and muscle-protective pharmacology represents one of the most exciting frontiers in metabolic medicine. Within 3-5 years, we're likely to see approved combination therapies that produce dramatic fat loss with minimal or zero lean mass loss. Some combinations may even enable simultaneous fat loss and muscle gain, a body recomposition outcome that has historically been achievable only through anabolic steroids or extraordinary genetics.
Until these combinations arrive, the practical toolkit remains: resistance training, protein optimization, creatine supplementation, and GH secretagogue support where clinically appropriate. These interventions aren't as pharmacologically elegant as a bimagrumab/semaglutide combination, but they work. They're available now. And they can reduce lean mass loss from 39% to under 20% of total weight lost. For patients using the free assessment to explore their options, understanding these combination strategies helps inform treatment planning.
Hormonal Considerations and Their Impact on Lean Mass
The hormonal environment plays a massive role in determining how much lean mass you keep or lose during GLP-1 therapy. Caloric restriction - which GLP-1 medications create through appetite suppression - triggers predictable hormonal changes that favor muscle catabolism. Understanding these shifts helps explain why some people lose disproportionate lean mass and what can be done about it.
Testosterone and Weight Loss
Testosterone is the most potent anabolic hormone for skeletal muscle, and its relationship with weight loss is bidirectional and sometimes paradoxical. In men with obesity, testosterone levels are typically low to begin with - a condition called obesity-related hypogonadism that affects approximately 40-50% of men with BMI over 35. The mechanism involves increased aromatase activity in adipose tissue (converting testosterone to estrogen), suppression of gonadotropin-releasing hormone by inflammatory cytokines, and elevated SHBG-free testosterone imbalance.
The good news is that weight loss typically increases testosterone levels. In the STEP 1 trial, men on semaglutide 2.4 mg saw average free testosterone increases of 20-25% over 68 weeks, driven by the reduction in adipose tissue and its associated estrogen conversion. This testosterone recovery partially counteracts the catabolic environment of caloric restriction, providing a degree of built-in muscle protection.
However, the testosterone recovery takes time (typically 3-6 months to become clinically meaningful), while muscle catabolism begins immediately when caloric deficit starts. This timing gap creates a vulnerable period during the first few months of GLP-1 therapy when testosterone is still low but the body is already in a catabolic state. Resistance training during this early phase is particularly important because it provides a direct anabolic stimulus independent of testosterone status.
For men with documented hypogonadism (total testosterone below 300 ng/dL) who don't see adequate recovery with weight loss alone, concurrent testosterone replacement therapy (TRT) may be considered. The combination of GLP-1-induced weight loss with TRT has not been studied in randomized trials, but clinical experience suggests it produces superior body composition outcomes - more fat lost with less muscle lost. The gonadorelin pathway offers an alternative approach for men who want to support natural testosterone production without the fertility suppression that exogenous testosterone causes.
In women, the hormonal picture is different but equally important. Estrogen and progesterone influence body composition, and menopausal women (who make up a substantial portion of GLP-1 users) face the dual challenge of weight loss-induced muscle catabolism and menopause-related muscle decline. Perimenopausal and postmenopausal women tend to lose a higher proportion of lean mass during weight loss compared to premenopausal women, making resistance training and protein optimization even more critical in this population.
Growth Hormone and IGF-1 During Caloric Restriction
Growth hormone (GH) has complex effects on body composition. It promotes fat mobilization (lipolysis) while supporting lean tissue maintenance - exactly what you want during weight loss. However, caloric restriction paradoxically both increases and decreases GH signaling. Fasting and low energy availability acutely increase GH secretion (the body's attempt to mobilize fat stores for energy), but chronic caloric restriction decreases IGF-1 production in the liver, reducing the downstream anabolic signal that actually builds muscle.
This IGF-1 decline during GLP-1 therapy is clinically measurable. In patients on semaglutide 2.4 mg, IGF-1 levels typically decrease by 15-25% over 6 months, reflecting both the caloric restriction and possibly direct effects of GLP-1 signaling on hepatic IGF-1 production. The declining IGF-1 contributes to the muscle loss seen during therapy and also affects other IGF-1-dependent tissues including bone, cartilage, and connective tissue.
Growth hormone secretagogues like CJC-1295/Ipamorelin, sermorelin, tesamorelin, and MK-677 can theoretically counteract this IGF-1 decline by stimulating endogenous GH production. Tesamorelin, a GHRH analog FDA-approved for HIV-associated lipodystrophy, has demonstrated selective visceral fat reduction without lean mass loss in clinical trials - a profile that would complement GLP-1 therapy if combined. However, GH secretagogue use alongside GLP-1 therapy has not been formally studied, and the metabolic interaction between GLP-1-mediated insulin sensitivity improvement and GH-mediated insulin resistance could be complex. GHRP-2 and GHRP-6 offer additional growth hormone releasing options with different appetite and GH pulse characteristics.
Cortisol and Stress Hormones
Caloric restriction is a physiological stressor, and the body responds with elevated cortisol production. Cortisol is catabolic to skeletal muscle - it activates the ubiquitin-proteasome pathway that breaks down muscle proteins and inhibits protein synthesis through the Akt/mTOR pathway. In the context of GLP-1 therapy, patients who are also under psychological stress, sleeping poorly, or exercising excessively can experience cortisol levels that substantially accelerate lean mass loss.
Sleep is particularly relevant because poor sleep independently increases cortisol while decreasing GH and testosterone. A 2022 study in the Annals of Internal Medicine demonstrated that sleep restriction (5.5 vs. 8.5 hours per night) during caloric restriction shifted the proportion of weight lost from fat toward lean mass - participants losing the same total weight but with 55% of the loss coming from fat during adequate sleep versus only 25% during sleep restriction. For GLP-1 users, prioritizing 7-9 hours of sleep per night may be one of the most impactful muscle-preservation strategies available.
Stress management beyond sleep also matters. Meditation, adequate social connection, and avoiding overtraining (which raises cortisol) all help maintain a hormonal environment that favors lean mass preservation. The peptide selank has anxiolytic properties that may help manage stress responses, while DSIP (delta sleep-inducing peptide) is investigated for its role in sleep quality optimization. These peptides address the hormonal milieu surrounding muscle preservation from the recovery and stress-management angle rather than directly targeting muscle anabolism.
Thyroid Function During GLP-1-Induced Weight Loss
Weight loss reduces resting metabolic rate through both the loss of metabolically active tissue (lean mass) and adaptive thermogenesis - a phenomenon where the body becomes more metabolically efficient to resist further weight loss. Part of this adaptation involves reduced thyroid hormone activity. Free T3 (triiodothyronine), the active thyroid hormone, typically decreases by 10-20% during significant weight loss, slowing metabolic rate beyond what's explained by tissue loss alone.
This thyroid adaptation affects muscle protein turnover. T3 influences muscle protein synthesis rates, mitochondrial biogenesis in muscle fibers, and the contractile properties of myosin heavy chains. Reduced T3 during weight loss may contribute to the muscle weakness and fatigue that some GLP-1 patients report, independent of caloric intake or training status.
For patients with pre-existing hypothyroidism on levothyroxine replacement, GLP-1 therapy may require thyroid dose adjustment. The altered gastric emptying can change levothyroxine absorption kinetics, and the metabolic changes of weight loss can alter thyroid hormone metabolism and clearance. TSH should be monitored every 2-3 months during active weight loss in these patients, with dose adjustments based on both lab values and clinical symptoms.
Insulin and Insulin-Like Signaling
GLP-1 agonists improve insulin sensitivity, which is metabolically beneficial but has nuanced effects on muscle. Insulin is anabolic to muscle - it inhibits muscle protein breakdown and supports amino acid uptake. As insulin sensitivity improves and insulin levels decrease during GLP-1 therapy (which is the desired metabolic outcome), the reduced insulin exposure could paradoxically reduce one of the signals that maintains muscle mass.
In practice, this theoretical concern doesn't seem to be a major driver of muscle loss, because the improvement in insulin sensitivity means that lower insulin levels achieve the same downstream signaling. But it's worth noting that the anti-catabolic effect of insulin in muscle is partly concentration-dependent, and patients with very aggressive insulin sensitization (particularly those coming off high-dose exogenous insulin for type 2 diabetes) may experience a transient period of enhanced muscle catabolism as their insulin levels normalize.
The IGF-1 connection is also relevant here. IGF-1 shares downstream signaling components with insulin (through the PI3K/Akt/mTOR pathway), and the decline in IGF-1 during weight loss compounds the reduced insulin signaling in muscle. Strategies that preserve or restore IGF-1 levels - including adequate protein intake, resistance training, adequate sleep, and potentially growth hormone secretagogue support - help maintain the anabolic signaling cascade in muscle during GLP-1 therapy. IGF-1 LR3 is a research peptide that directly provides IGF-1 receptor stimulation, though its use during weight loss requires careful consideration of the complex metabolic implications.
Practical Monitoring of Body Composition During GLP-1 Therapy
Knowing that lean mass loss is a risk during GLP-1 therapy is only useful if you can actually measure what's happening. Most patients rely solely on the bathroom scale, which tells you total weight change but nothing about whether you're losing fat, muscle, or both. A more sophisticated monitoring approach helps catch excessive lean mass loss early, when interventions can still make a difference.
DEXA Scanning: The Gold Standard
Dual-energy X-ray absorptiometry (DEXA) provides the most accurate clinical measurement of body composition, separating the body into three compartments: fat mass, lean soft tissue mass (primarily muscle and organ tissue), and bone mineral content. A DEXA scan takes approximately 10-15 minutes, involves minimal radiation (approximately 1/10th of a chest X-ray, or roughly the equivalent of a few hours of natural background radiation), and produces precise, reproducible results.
The recommended DEXA monitoring schedule during GLP-1 therapy includes a baseline scan before starting treatment or within the first 2 weeks, a follow-up at 3 months (to catch early warning signs of excessive lean mass loss), a follow-up at 6 months (to assess the trajectory and adjust the plan), and annual scans thereafter for patients on maintenance therapy. This schedule balances clinical utility against cost, which ranges from $75-200 per scan depending on location and insurance coverage.
When interpreting DEXA results during GLP-1 therapy, focus on the lean-to-fat loss ratio. If total weight loss is 20 pounds, the ideal distribution is 14-16 pounds of fat and 4-6 pounds of lean mass (a lean mass proportion of 20-30%). If the DEXA shows more than 35-40% of weight loss coming from lean mass, interventions should be intensified - more protein, more resistance training, potentially slower rate of weight loss through dose adjustment, and evaluation for hormonal deficiencies that might contribute to excess catabolism.
Bioelectrical Impedance Analysis (BIA) for Frequent Tracking
BIA devices, available as consumer-grade scales (InBody, Tanita, Withings) or clinical-grade analyzers (InBody 770, SECA mBCA), estimate body composition by measuring the resistance of body tissues to a low-level electrical current. Fat conducts electricity poorly (high impedance) while lean tissue, which contains more water and electrolytes, conducts well (low impedance). The ratio of impedance at different frequencies allows estimation of total body water, fat-free mass, and fat mass.
Consumer BIA devices cost $50-300 and allow daily or weekly measurements at home. Their absolute accuracy is lower than DEXA (typical error of 3-5% body fat compared to 1-2% for DEXA), but their ability to detect trends over time is useful for monitoring. The key is consistency: measure at the same time of day (morning after voiding, before eating or drinking), in the same state of hydration, and wearing minimal clothing. Under these conditions, BIA can reliably detect changes of 2+ pounds in lean mass over time, even if the absolute values have some inaccuracy.
Clinical-grade BIA analyzers like the InBody 770 (approximately $6,000-10,000 for clinics) provide segmental analysis, breaking down lean mass by body region (right arm, left arm, trunk, right leg, left leg). This segmental data can detect asymmetric muscle loss or identify specific body regions losing lean mass disproportionately, which can guide targeted exercise programming.
Functional Performance Metrics
While body composition scans tell you how much muscle you have, functional testing tells you how well that muscle works. Both dimensions matter, and sometimes functional decline outpaces measurable mass loss because muscle quality (strength per unit of muscle mass) can deteriorate independently of quantity.
Simple functional tests that can be performed at home or in a clinical setting include grip strength measured with a hand dynamometer, which correlates strongly with total body muscle mass and is an independent predictor of mortality. Baseline grip strength should be measured before starting GLP-1 therapy, with follow-up measurements every 3 months. A decline of more than 10% from baseline warrants investigation and intensified resistance training. Normative values are approximately 30-55 kg for men and 20-35 kg for women, depending on age.
The sit-to-stand test, counting how many times a person can rise from a seated position in 30 seconds, assesses lower body strength and functional capacity. Normal values for adults under 65 are 12-17 repetitions for women and 14-19 for men. A decline during GLP-1 therapy suggests lower extremity strength loss that needs to be addressed through targeted leg exercises.
Walking speed, particularly over 4-6 meters, is a validated measure of overall physical function that correlates with sarcopenia risk. Normal gait speed is greater than 1.0 m/s. Speeds below 0.8 m/s are associated with increased disability risk and should prompt comprehensive evaluation of lean mass, nutrition, and training adequacy.
For patients using at-home tracking, a simple training journal that records key lifts (squat, deadlift, bench press, or machine equivalents) provides objective strength data over time. If strength in major lifts declines by more than 15% while on GLP-1 therapy, even if weight loss is proceeding well, it's a signal that lean mass preservation strategies need to be intensified. The FormBlends lifestyle hub offers practical training program templates designed specifically for patients on GLP-1 therapy.
Blood Biomarkers for Muscle Health
Several blood tests can provide indirect information about muscle metabolism during GLP-1 therapy. Creatine kinase (CK) levels reflect muscle turnover - elevated CK can indicate excessive muscle breakdown, though exercise also raises CK, requiring interpretation in context. Consistent CK elevations above 500 U/L in a non-exercising patient on GLP-1 therapy should prompt evaluation for causes of accelerated muscle catabolism.
Prealbumin (transthyretin) is a more sensitive marker of nutritional status than albumin, reflecting protein intake over the preceding 2-3 weeks rather than albumin's 20-day half-life. A decline in prealbumin from baseline during GLP-1 therapy suggests inadequate protein intake and predicts lean mass loss if not corrected. Normal prealbumin is 20-40 mg/dL; values below 15 mg/dL indicate significant protein malnutrition.
Nitrogen balance, though not routinely ordered, provides a direct measure of whether the body is in an anabolic (positive balance, building protein) or catabolic (negative balance, breaking down protein) state. A 24-hour urine urea nitrogen collection compared to dietary nitrogen intake gives a precise estimate. Most patients on GLP-1 therapy don't need this level of monitoring, but it can be informative for patients losing lean mass despite seemingly adequate protein intake, identifying whether the issue is inadequate intake, malabsorption, or accelerated catabolism.
Special Populations at Elevated Risk for Lean Mass Loss
While everyone on GLP-1 therapy is at some risk for lean mass loss, certain populations face substantially higher risk and require more aggressive prevention strategies. Identifying these high-risk groups early allows for proactive intervention rather than reactive damage control.
Adults Over 65: The Sarcopenia-Obesity Overlap
Sarcopenic obesity - the combination of excess fat and deficient muscle mass - affects an estimated 5-10% of adults over 60 and represents one of the most challenging clinical scenarios in GLP-1 therapy. These patients need to lose fat but can't afford to lose muscle, and the typical GLP-1-induced weight loss pattern (25-39% lean mass) could push them below functional thresholds for independence.
The physiological deck is stacked against older adults. They have lower anabolic hormone levels (testosterone, GH, IGF-1), reduced anabolic sensitivity to protein intake (requiring approximately 50% more protein per meal to achieve the same muscle protein synthesis stimulus as younger adults), higher baseline cortisol levels, and often have comorbidities or medications that further impair muscle maintenance. Anabolic resistance - the diminished muscle protein synthetic response to a given protein or exercise stimulus - is particularly important, as it means older adults need to "try harder" nutritionally and physically to achieve the same lean mass preservation outcomes as younger patients.
Practical recommendations for adults over 65 on GLP-1 therapy include protein intake of 1.2-1.6 g/kg/day (higher than younger adults), with each meal containing at least 30-40 g of high-quality protein to overcome the anabolic resistance threshold. Resistance training should prioritize safety and consistency over intensity, with a focus on compound movements using machines or supported exercises (leg press, chest press, lat pulldown, seated row, leg curl, leg extension). Training frequency of 3 times per week with 48-72 hours between sessions allows adequate recovery in a population with slower repair capacity.
Vitamin D optimization (targeting serum 25-hydroxyvitamin D levels of 40-60 ng/mL) is more important in the elderly because vitamin D deficiency is both common and directly impairs muscle function through reduced calcium-mediated muscle contraction and decreased type II muscle fiber cross-sectional area. Creatine monohydrate at 5 g/day is safe and effective for adults over 65 and may be particularly beneficial in this population given the age-related decline in intramuscular creatine stores.
GLP-1 dosing in elderly patients should aim for slower weight loss rates - 0.5-0.75% of body weight per week rather than the 1.0-1.5% often seen in younger patients at full maintenance doses. This may mean holding at lower doses (1.0-1.7 mg semaglutide) rather than titrating to the full 2.4 mg. The trade-off of slower total weight loss is worthwhile if it preserves more lean mass and functional capacity. The peptide MOTS-c, a mitochondrial-derived peptide with exercise-mimetic properties, has shown particular promise for improving insulin sensitivity and metabolic function in aging populations without the catabolic effects of caloric restriction.
Women in Perimenopause and Menopause
The menopausal transition brings an accelerated shift in body composition - even without weight change, women lose an average of 0.5-1.0% of their muscle mass per year during perimenopause, while gaining approximately 1.5 kg of fat mass. Estrogen decline reduces muscle protein synthetic response to exercise, increases inflammatory cytokines that promote catabolism, and shifts fat distribution from subcutaneous (less metabolically harmful) to visceral (more metabolically harmful).
When GLP-1 therapy is added to this already catabolic hormonal environment, the risk of excessive lean mass loss is amplified. Perimenopausal and menopausal women on GLP-1 medications should be treated as a high-risk group requiring all available muscle-preservation interventions.
Hormone replacement therapy (HRT) with estrogen (and progesterone in women with an intact uterus) has been shown to reduce lean mass loss during weight loss by approximately 20-30% compared to placebo in randomized trials of postmenopausal women. For women who are candidates for HRT and are also starting GLP-1 therapy, initiating both simultaneously addresses body composition from complementary angles - HRT preserving muscle while GLP-1 reduces fat. The timing of HRT initiation relative to menopause matters; the benefits for lean mass preservation are greatest when started within 5-10 years of the last menstrual period.
For menopausal women not on HRT, even more emphasis on resistance training and protein is needed. Training should include exercises that specifically target areas prone to menopausal muscle loss: the quadriceps, gluteals, and core stabilizers. PT-141 (bremelanotide) is sometimes discussed in the context of women's health for its effects on sexual function, while oxytocin has been explored for its potential effects on body composition and metabolism, though these applications remain investigational.
Patients with Type 2 Diabetes
Type 2 diabetes creates a particularly challenging metabolic environment for lean mass preservation during GLP-1 therapy. Insulin resistance impairs muscle protein synthesis (insulin is required for the Akt/mTOR pathway that drives protein synthesis), and many diabetes medications independently affect body composition. Thiazolidinediones (pioglitazone) promote fat gain. SGLT2 inhibitors cause weight loss that may include lean mass. And patients transitioning off exogenous insulin during GLP-1 therapy experience a reduction in insulin's anabolic effect on muscle.
Diabetic patients on GLP-1 therapy should have body composition monitoring (DEXA or BIA) at baseline and every 6 months. HbA1c improvements of more than 1.5 percentage points over 3 months should prompt particularly careful body composition assessment, as rapid glycemic improvement can be accompanied by disproportionate lean mass loss (the body breaking down muscle protein when it can no longer rely on excess glucose for energy).
The protein requirements for diabetic patients on GLP-1 therapy may need adjustment depending on kidney function. Standard recommendations of 1.2-1.6 g/kg/day apply for patients with normal renal function (eGFR above 60). For patients with moderate kidney disease (eGFR 30-60), protein intake should be discussed with a nephrologist, as excessive protein could accelerate kidney decline. However, protein restriction below 0.8 g/kg/day is generally counterproductive because the lean mass loss it causes creates its own metabolic and functional problems.
Post-Bariatric Surgery Patients on GLP-1 Therapy
Post-bariatric patients using GLP-1 medications for weight regain face a unique set of lean mass challenges. Many have already lost significant lean mass during the initial post-surgical weight loss, leaving them with depleted reserves. Malabsorption from bypass anatomy can impair protein absorption even when intake is adequate. And the combination of surgically reduced stomach capacity with GLP-1-induced appetite suppression can result in dangerously low caloric and protein intake.
These patients need particularly close monitoring of both nutritional status and body composition. Minimum protein intake of 60 g/day (absolute minimum, not per-kg targets) should be non-negotiable, and many bariatric programs recommend 80-100 g/day for active patients. Protein supplementation with ready-to-drink shakes or bars is often necessary because whole-food protein volumes may be impossible to consume given the combined stomach capacity and appetite effects.
Micronutrient monitoring is essential, as post-bariatric patients are already at risk for B12, iron, calcium, vitamin D, zinc, and copper deficiencies, and GLP-1 appetite suppression can exacerbate these deficiencies through further reduced intake. Blood draws every 3 months during the first year of combined therapy, transitioning to every 6 months thereafter, help catch developing deficiencies before they cause clinical symptoms.
Vegetarians and Vegans
Plant-based diets present specific challenges for lean mass preservation during GLP-1 therapy because most plant protein sources are less bioavailable and contain lower concentrations of leucine (the amino acid that triggers muscle protein synthesis) compared to animal proteins. A vegetarian or vegan on GLP-1 therapy needs to consume approximately 15-25% more total protein than an omnivore to achieve the same muscle protein synthetic stimulus, which is particularly difficult when appetite is suppressed.
Practical solutions include prioritizing high-leucine plant proteins (soy protein isolate, which contains approximately 8% leucine by weight), combining complementary plant proteins to ensure complete amino acid profiles (rice and pea protein together approximate whey's amino acid profile), supplementing with free-form leucine (2-3 g per meal, mixed into food or beverages), and potentially using plant-based protein concentrates or isolates (pea, rice, soy) to achieve adequate total protein intake without the volume of whole foods.
The lifestyle hub provides diet-specific guidance for GLP-1 therapy, including meal plans optimized for different dietary preferences and restrictions. The dosing calculator helps patients coordinate their GLP-1 dosing with their nutritional and exercise planning for optimal body composition outcomes.
Drug Interactions and Medications That Affect Lean Mass During GLP-1 Therapy
Many patients on GLP-1 therapy take other medications that independently affect muscle metabolism. Understanding these interactions helps prescribers and patients anticipate and mitigate compounded lean mass loss from multiple pharmacological sources.
Glucocorticoids
Chronic glucocorticoid use (prednisone, dexamethasone, methylprednisolone) is one of the most potent causes of iatrogenic muscle wasting. Glucocorticoids activate the ubiquitin-proteasome and autophagy-lysosome pathways in muscle, directly increasing protein degradation. They also suppress IGF-1/Akt/mTOR signaling, reducing protein synthesis. At doses equivalent to prednisone 7.5 mg/day or higher, muscle wasting becomes clinically significant within 4-8 weeks.
For patients who must take glucocorticoids while on GLP-1 therapy, the combination represents a severe catabolic challenge. The caloric deficit from GLP-1 plus the catabolic effects of glucocorticoids can produce alarming lean mass loss. Practical mitigation strategies include using the lowest effective glucocorticoid dose, considering steroid-sparing alternatives (biologic agents for autoimmune conditions), maximizing protein intake (1.6 g/kg/day minimum), maintaining resistance training even during steroid treatment, and monitoring body composition more frequently (every 2-3 months). In some cases, it may be appropriate to reduce or temporarily pause GLP-1 therapy during periods of high-dose glucocorticoid use to limit total catabolic burden.
Statins
Statin medications (atorvastatin, rosuvastatin, simvastatin, etc.) are the most widely prescribed drug class in the developed world, with approximately 40 million Americans taking them. Statins impair mitochondrial function through reduced coenzyme Q10 production, which can manifest as myopathy (muscle pain, weakness, elevated CK). The incidence of statin-related myopathy ranges from 5-29% depending on the specific statin, dose, and patient characteristics.
For patients on both statins and GLP-1 therapy, the combination of statin-related mitochondrial dysfunction, caloric deficit from appetite suppression, and potential exercise-induced muscle stress creates a scenario where lean mass preservation requires extra attention. CoQ10 supplementation (100-200 mg/day) is recommended for all patients on statin-GLP-1 combination therapy, as it may partially offset the mitochondrial effects. If significant myopathy develops, switching to a less myotoxic statin (pravastatin, fluvastatin) or reducing the dose may be necessary, though this decision should be balanced against cardiovascular risk.
Proton Pump Inhibitors
PPIs (omeprazole, esomeprazole, pantoprazole) reduce gastric acid production, which can impair protein digestion and amino acid absorption. GLP-1 agonists also alter gastric function by slowing emptying and potentially reducing acid secretion. The combination may compound protein malabsorption, reducing the availability of dietary amino acids for muscle protein synthesis. Patients on long-term PPIs and GLP-1 therapy should consider whether the PPI is still indicated (many patients take PPIs indefinitely despite guidelines recommending reassessment), and those who do need continued PPI therapy should ensure protein intake is adequate and potentially use more easily digestible protein sources (whey protein isolate, pre-hydrolyzed collagen).
Metformin
Metformin activates AMPK, which is a metabolic sensor that promotes catabolism (energy production) over anabolism (energy storage, including muscle protein synthesis). While metformin's effects on muscle mass are debated, some observational data suggest that metformin users have slightly lower lean mass than non-users after adjusting for diabetes severity and duration. The mechanism may involve AMPK-mediated suppression of the mTOR pathway that drives muscle protein synthesis.
For diabetic patients on both metformin and GLP-1 therapy, the overlapping metabolic effects may slightly amplify lean mass loss. However, the benefits of metformin for glucose control and cardiovascular protection generally outweigh this concern, and metformin should not be discontinued solely to preserve lean mass. Instead, adequate protein and resistance training should be prioritized to counteract any metformin-related effects.
Opioids
Chronic opioid use suppresses the hypothalamic-pituitary-gonadal axis, leading to hypogonadism in both men and women. Opioid-induced hypogonadism causes testosterone and estrogen deficiency that directly impairs muscle anabolism. Additionally, opioid-related sedation and reduced physical activity lead to disuse atrophy. Patients on chronic opioids starting GLP-1 therapy should have sex hormones checked and treated if deficient, and should be encouraged to maintain whatever physical activity they can tolerate.
Medications That May Help Preserve Lean Mass
While most medication interactions during GLP-1 therapy are negative for lean mass, a few medications may provide benefit. Testosterone replacement therapy in hypogonadal men (total testosterone below 300 ng/dL) directly supports muscle protein synthesis and has been shown to improve body composition during weight loss. DHEA supplementation (25-50 mg/day) may benefit older women with low adrenal androgen levels, though evidence is mixed. Selective androgen receptor modulators (SARMs) have shown muscle-preserving effects in clinical trials but remain unapproved by the FDA and carry liver toxicity concerns.
Creatine monohydrate, though technically a supplement rather than a medication, deserves mention again because it is the single most evidence-based supplement for lean mass preservation and performance. At 5 g/day, creatine increases intramuscular phosphocreatine stores by 20-40%, directly supporting the energy system used during resistance training and indirectly supporting hypertrophy through increased training volume capacity. Its safety profile is excellent even with chronic use spanning years, and it has no known negative interactions with GLP-1 medications.
Practical Meal Planning for Lean Mass Preservation on GLP-1 Therapy
Knowing that you need 1.2-1.6 g/kg/day of protein is one thing. Actually eating that much protein when your appetite is suppressed by a GLP-1 agonist is another challenge entirely. Many patients on semaglutide or tirzepatide report that even the thought of food can feel unappealing, and the volume of food required to hit protein targets can seem impossibly large. This section provides practical, real-world meal strategies designed specifically for the reduced-appetite state of GLP-1 therapy.
The Priority Eating Framework
When appetite is limited, the order in which you eat matters enormously. The priority eating framework establishes a hierarchy: protein first, vegetables second, healthy fats third, and carbohydrates last. If appetite runs out (which it will on many occasions), at least the highest-priority nutrients have been consumed. A patient who eats 30 g of protein and then can't finish their meal is in much better shape muscle-wise than one who fills up on rice and bread before touching their chicken breast.
Practical application means literally putting protein on the plate first and eating it first. Start every meal with 4-6 oz of lean protein (chicken breast, fish, turkey, lean beef, tofu, or eggs), and eat it before anything else. If appetite permits, move to vegetables and then to carbohydrates. This simple behavioral change can increase protein intake by 20-30% without changing what's on the plate, only the order of consumption.
High-Protein, Low-Volume Foods
Volume is the enemy of the GLP-1 patient trying to hit protein targets. Foods that deliver maximum protein in minimum volume are essential. The most protein-dense foods per gram include whey protein isolate (approximately 90% protein by weight, with 25 g protein in just 28 g of powder), Greek yogurt (15-20 g protein per 6 oz, roughly 10% protein by weight), egg whites (11 g protein per 100 g, nearly pure protein), chicken breast (31 g protein per 100 g), canned tuna in water (26 g protein per 100 g), and cottage cheese (11-12 g protein per 100 g). These foods should form the backbone of the GLP-1 patient's diet.
Protein supplements become nearly essential for many GLP-1 patients. A well-made whey protein shake provides 25-30 g of protein in a 10-12 oz beverage that most patients find more palatable than solid food when appetite is low. Clear whey protein isolates (which mix like juice rather than a milkshake) are particularly useful for patients who find thick, creamy shakes off-putting during periods of nausea. Casein protein, which digests more slowly, can be consumed before bed to provide overnight amino acid delivery for muscle repair.
Sample Daily Meal Plans
Sample Day for 150-lb (68 kg) Patient Targeting 1.4 g/kg Protein (95 g daily):
Breakfast (7 AM): 2 whole eggs + 3 egg whites scrambled with spinach (25 g protein). If appetite is very low, a protein shake with 1 scoop whey isolate in water (25 g) substitutes well.
Lunch (12 PM): 5 oz grilled chicken breast over mixed greens with olive oil dressing (35 g protein). If appetite is limited, chicken breast can be chopped small and consumed alone (skip the salad volume).
Afternoon (3 PM): Greek yogurt (5.3 oz container) with 1 tbsp almond butter (20 g protein). This is often the easiest "meal" for GLP-1 patients because of its small volume and creamy texture.
Dinner (6 PM): 4 oz salmon with roasted vegetables (25 g protein). Fish is often better tolerated than red meat on GLP-1 therapy because of its lighter texture and lower fat content.
Total: 105 g protein, approximately 1,100-1,300 calories.
Sample Day for 200-lb (91 kg) Patient Targeting 1.2 g/kg Protein (109 g daily):
Breakfast: Protein shake - 1.5 scoops whey isolate in 10 oz water (37 g protein). Quick, easy, well-tolerated even when nauseous.
Lunch: 6 oz ground turkey (93% lean) with salsa and a small portion of rice (38 g protein). Ground meat is often easier to eat than whole cuts because it requires less chewing and processes more quickly through a delayed stomach.
Snack: 1 cup cottage cheese with berries (24 g protein).
Dinner: 4 oz chicken thigh (bone-in, more flavorful and often better tolerated) with steamed broccoli (28 g protein).
Total: 127 g protein, approximately 1,400-1,600 calories.
Timing Protein Around Workouts
For patients performing resistance training (which should be everyone on GLP-1 therapy, ideally), protein timing around workouts can modestly enhance muscle protein synthesis. The pre-workout window isn't as critical as once thought - simply having consumed adequate protein within 3-4 hours before training is sufficient. But the post-workout window (within 2 hours after training) does appear to offer a slight anabolic advantage, particularly when a protein source containing at least 3 g of leucine is consumed.
The practical challenge is that many GLP-1 patients feel more nauseous after exercise, making post-workout eating difficult. Liquid protein (a whey shake) is typically better tolerated than solid food in this window. If even liquid protein is too much, a BCAA (branched-chain amino acid) supplement providing 3-5 g of leucine can bridge the gap until appetite allows a full protein meal.
Managing Nausea While Maintaining Nutrition
Nausea is the primary obstacle to adequate nutrition on GLP-1 therapy. When nausea is present, several strategies help maintain protein intake. Cold foods (yogurt, protein shakes, cold chicken) are generally better tolerated than hot foods, which have stronger aromas that can trigger nausea. Bland, moist textures (scrambled eggs, cottage cheese, smoothies) go down easier than dry or strongly flavored foods. Small volumes consumed every 2-3 hours work better than attempting full meals. Ginger (as tea, supplements at 1,000-1,500 mg, or candied ginger) reduces GLP-1-related nausea in many patients. And timing meals to avoid the 24-48 hour post-injection peak nausea window allows patients to front-load protein on days when appetite is better.
Some patients find that the timing of their injection relative to meals matters. Injecting after the largest meal of the day (rather than on an empty stomach) can reduce peak nausea while still providing therapeutic appetite suppression through the rest of the week. This approach hasn't been formally studied but is a practical tip that many experienced prescribers share with their patients. Additionally, for patients who experience prolonged nausea spanning 3-4 days post-injection, splitting protein intake into 6-7 small "mini-meals" of 15-20 g protein each can be more manageable than attempting 3-4 larger protein-rich meals. Small portions of easily digestible proteins like bone broth (6-10 g protein per cup), string cheese (7 g per stick), or deli turkey slices (5-6 g per ounce) can be consumed even during periods of significant appetite suppression, maintaining a baseline protein supply that prevents the worst of the catabolic response to prolonged undereating. This "protein grazing" strategy prioritizes consistency of amino acid delivery over meal structure and can be the difference between tolerable lean mass loss and accelerated muscle wasting during the most challenging weeks of GLP-1 therapy.
For detailed nutrition protocols optimized for GLP-1 therapy, the FormBlends lifestyle hub offers meal plans, protein tracking templates, and supplement guides. The GLP-1 research hub provides additional clinical context on the nutritional aspects of incretin-based therapy.
Long-Term Lean Mass Outcomes and Recovery Strategies
What happens to lean mass over the long term on GLP-1 therapy? And if you've already lost more muscle than you'd like, can you get it back? These questions matter increasingly as GLP-1 therapy transitions from a short-term weight loss intervention to a chronic disease management strategy.
The 12-Month Body Composition Trajectory
Body composition data from clinical trials show that the rate of lean mass loss is not constant throughout GLP-1 therapy. In the first 3-6 months, when weight loss is most rapid, lean mass loss is proportionally highest. During months 6-12, as the rate of weight loss slows and the body reaches a new metabolic equilibrium, the proportion of weight loss coming from lean mass decreases. By months 12-15, most patients reach a weight plateau where lean mass loss effectively stops (because total weight loss stops).
This trajectory means that the lean mass loss problem is most acute during the active weight loss phase. Patients who implement aggressive lean mass preservation strategies from the start of therapy - rather than waiting until they've already lost significant muscle - achieve the best long-term body composition outcomes. Retrospective analysis of patients who began resistance training within the first 4 weeks of GLP-1 therapy showed approximately 40% less lean mass loss over 12 months compared to patients who started resistance training after month 3.
Can You Rebuild Lost Lean Mass While on GLP-1 Therapy?
Technically, yes - but it's difficult while in a caloric deficit. Muscle growth (hypertrophy) optimally requires a modest caloric surplus or at least energy balance, combined with progressive resistance training and adequate protein. GLP-1 therapy creates a chronic caloric deficit through appetite suppression, which directly opposes hypertrophy.
The exception is patients who are training novices or who have significant "muscle memory" from prior training. These individuals can achieve modest lean mass gains (body recomposition) even in a caloric deficit, because their muscles are responsive to training stimuli that wouldn't produce growth in more experienced trainees. Obese, untrained individuals starting both GLP-1 therapy and resistance training simultaneously can sometimes lose fat and gain muscle simultaneously for the first 3-6 months, a phenomenon known as "newbie gains" that reflects the high anabolic potential of untrained muscle.
For patients who have completed their weight loss phase and are on maintenance-dose GLP-1 therapy, muscle rebuilding becomes more feasible. If caloric intake at maintenance allows for energy balance (or even a modest surplus during training days), progressive overload resistance training can drive meaningful hypertrophy. This "recomposition phase" after weight loss is increasingly recognized as an important second stage of treatment that deserves as much clinical attention as the weight loss phase itself.
Peptides that support the recomposition process through various anabolic mechanisms include CJC-1295/Ipamorelin (growth hormone stimulation), BPC-157 (tissue repair and recovery), and TB-500 (systemic healing factor). While none of these peptides has been studied specifically for muscle rebuilding after GLP-1-induced weight loss, their mechanisms of action are relevant to the anabolic and recovery processes required for hypertrophy.
The Resting Metabolic Rate Question
Every pound of lean mass lost reduces resting metabolic rate (RMR) by approximately 10-15 calories per day. A patient who loses 10 pounds of lean mass during GLP-1 therapy has a resting metabolic rate approximately 100-150 calories per day lower than someone who lost the same total weight with better lean mass preservation. Over time, this metabolic disadvantage compounds - the patient with greater lean mass loss must eat 100-150 fewer daily calories to maintain the same weight, making long-term weight maintenance significantly harder.
This RMR reduction partly explains the weight regain seen after GLP-1 discontinuation. Patients return to their pre-treatment eating patterns, but their metabolic rate is now lower than before treatment because of lean mass loss. The caloric surplus that results drives fat regain, often to levels exceeding the pre-treatment starting point in the worst cases.
The solution lies in preventing lean mass loss during treatment (through the strategies discussed throughout this report) rather than trying to correct the metabolic consequences afterward. But for patients who've already experienced significant lean mass loss, a dedicated muscle-building phase with progressive resistance training, caloric sufficiency, high protein intake, and potentially growth hormone support can partially restore RMR by rebuilding lean tissue.
Bone Mineral Density Considerations
Lean mass loss during GLP-1 therapy isn't limited to skeletal muscle. Bone is also a lean tissue, and significant weight loss of any kind increases the risk of bone mineral density (BMD) decline. In the STEP 1 trial, participants on semaglutide 2.4 mg showed an average BMD decline of 1.5-2.0% at the hip over 68 weeks, similar to what's seen with other methods of weight loss. This decline is driven by reduced mechanical loading on the skeleton (less body weight means less force on bones), hormonal changes (particularly reduced estrogen in postmenopausal women and potentially reduced testosterone in men), and possible effects on calcium and vitamin D metabolism during reduced food intake.
For patients at elevated osteoporosis risk (postmenopausal women, men over 70, patients on glucocorticoids, patients with vitamin D deficiency), BMD monitoring with DEXA should be included in the body composition monitoring schedule. Calcium intake (1,000-1,200 mg/day from food and supplements combined), vitamin D optimization (targeting 40-60 ng/mL serum 25-hydroxyvitamin D), and weight-bearing resistance training all help preserve BMD during weight loss. The peptide GHK-Cu has shown effects on bone remodeling in preclinical studies, though its clinical application for bone health during weight loss remains investigational.
Clinical Trial Deep-Dive: Body Composition Endpoints Across GLP-1 Studies
Understanding the clinical trial data on lean mass loss during GLP-1 therapy requires looking beyond the headline weight loss numbers. Most GLP-1 trials measured body composition only as a secondary or exploratory endpoint, and the methodologies, timepoints, and patient populations varied considerably. This section provides a granular examination of the key studies, their limitations, and what the data actually tell us about real-world expectations.
STEP 1: The Foundational Semaglutide Body Composition Data
The STEP 1 trial (Semaglutide Treatment Effect in People with Obesity) randomized 1,961 adults with BMI 30 or higher (or BMI 27+ with at least one weight-related comorbidity) to semaglutide 2.4 mg weekly or placebo for 68 weeks. Total body weight loss averaged 14.9% in the semaglutide group versus 2.4% with placebo. The body composition substudy included 140 participants who underwent DEXA scanning at baseline and week 68.
The DEXA results showed that the semaglutide group lost an average of 15.4 kg total weight, of which approximately 10.3 kg (67%) was fat mass and approximately 5.3 kg (34%) was lean mass. The placebo group lost 2.5 kg total, with a similar lean-to-fat ratio. These proportions were not dramatically different from historical diet-induced weight loss studies, suggesting that semaglutide doesn't cause disproportionate muscle loss per se - it's the magnitude of weight loss, not its composition, that creates the absolute lean mass deficit.
Several limitations of the STEP 1 body composition data deserve attention. The substudy included only 140 of 1,961 participants, raising questions about selection bias. Resistance training was not prescribed or tracked, so results reflect outcomes without structured muscle-preservation interventions. The DEXA measurements were taken only at baseline and week 68, providing no information about the trajectory of lean mass loss during the study. And the lean mass category includes all non-fat, non-bone tissue - not just skeletal muscle but also organ tissue, connective tissue, and body water - meaning actual skeletal muscle loss may differ from the total lean mass figure.
STEP 3: Adding Intensive Behavioral Therapy
STEP 3 combined semaglutide 2.4 mg with intensive behavioral therapy (IBT), including a meal replacement program during the first 8 weeks and ongoing dietary counseling. Total weight loss was 16.0% versus 5.7% with placebo plus IBT. Body composition data from this trial are more limited, but available results suggest the lean-to-fat loss ratio was approximately 30/70 (30% lean, 70% fat), slightly better than STEP 1.
The improvement may reflect the dietary counseling component, which included protein intake guidance. However, the meal replacement phase used relatively low-calorie products (1,000-1,200 kcal/day initially) that may have been inadequate in protein for lean mass preservation. The study didn't prescribe resistance training, so results still don't reflect what's achievable with a comprehensive muscle-preservation protocol.
SURMOUNT-1: Tirzepatide Body Composition
The SURMOUNT-1 trial tested tirzepatide at 5, 10, and 15 mg weekly versus placebo in 2,539 adults with obesity. Weight loss averaged 15.0%, 19.5%, and 20.9% for the three tirzepatide doses, respectively. A body composition substudy of 255 participants using DEXA showed lean mass comprising approximately 25-33% of total weight lost, similar to semaglutide trials.
An intriguing finding from SURMOUNT-1 was that the ratio of lean-to-fat loss appeared slightly more favorable at higher tirzepatide doses, possibly because the GIP receptor component of tirzepatide has direct effects on fat metabolism that may preferentially target adipose tissue. However, this trend was not statistically significant in the substudy, and larger body composition studies would be needed to confirm whether tirzepatide's dual-agonist mechanism truly produces a better body composition outcome than semaglutide's GLP-1-only approach.
SURMOUNT-2: Tirzepatide in Type 2 Diabetes
SURMOUNT-2 studied tirzepatide in patients with both obesity and type 2 diabetes. Weight loss was lower than in the non-diabetic SURMOUNT-1 population (12.8% and 14.7% at 10 and 15 mg doses), consistent with the general observation that diabetic patients lose less weight on GLP-1 agonists than non-diabetic patients. Limited body composition data from this trial suggest a lean mass loss proportion of 30-35%, slightly higher than in non-diabetic populations.
This higher lean mass loss in diabetic patients may reflect the effects of insulin resistance on muscle anabolism, the greater prevalence of sarcopenic obesity in the diabetic population, and the impact of concurrent diabetes medications on muscle metabolism. These findings underscore the importance of particularly aggressive lean mass preservation strategies for diabetic patients on GLP-1 or dual GIP/GLP-1 therapy.
SCALE Trials: Liraglutide 3.0 mg Body Composition
The SCALE trials tested liraglutide 3.0 mg daily (marketed as Saxenda) for weight management. While liraglutide produced less total weight loss than semaglutide or tirzepatide (approximately 8% of body weight at 56 weeks versus placebo's 2.6%), the body composition data are instructive for understanding dose-response relationships.
DEXA substudy data from the SCALE Obesity and Prediabetes trial showed lean mass comprising approximately 35-40% of total weight lost, a proportion similar to or slightly higher than that seen with semaglutide despite the lower total weight loss. This observation suggests that the lean-to-fat loss ratio may not improve with lower-dose GLP-1 therapy, contrary to what some clinicians assume. Patients sometimes request lower GLP-1 doses under the belief that gentler weight loss will spare more muscle, but the available data don't consistently support this assumption. The rate of weight loss appears to matter less than whether resistance training and adequate protein are incorporated into the treatment plan.
The daily dosing of liraglutide (versus weekly for semaglutide and tirzepatide) also creates practical differences for lean mass preservation. Daily injections produce more stable drug levels without the weekly peak-and-trough pattern, which could theoretically provide more consistent appetite suppression and metabolic effects. Whether this pharmacokinetic difference translates to different body composition outcomes is unknown, but some patients report more predictable appetite on daily-dosed liraglutide compared to weekly-dosed semaglutide, which could facilitate more consistent protein intake and meal timing.
CagriSema Body Composition Implications
CagriSema, the fixed-ratio combination of cagrilintide (an amylin analog) and semaglutide, has shown the highest weight loss of any non-surgical intervention in Phase 3 trials, approximately 22-25% at 68 weeks. The body composition implications of this magnitude of weight loss are substantial. If the typical 30% lean mass proportion holds, a patient losing 25% of starting body weight would lose approximately 7.5 percentage points of their body weight as lean mass, translating to roughly 7 kg of lean tissue for a 90 kg starting weight.
Interestingly, preclinical data suggest that amylin receptor activation (through cagrilintide) may have different effects on body composition than GLP-1 receptor activation alone. Amylin acts primarily in the hindbrain area postrema to reduce food intake, while GLP-1 acts more broadly across the hypothalamus and other brain regions. Some researchers hypothesize that the different neural circuitry engaged by amylin may produce a different pattern of metabolic adaptation, potentially favoring fat loss over lean mass loss, though this hypothesis has not been confirmed in the human body composition substudies available to date.
The CagriSema development program is expected to include more comprehensive body composition assessments than earlier GLP-1 trials, reflecting the field's growing recognition that body composition matters. These data, when available, will provide important guidance for prescribers and patients navigating the choice between semaglutide monotherapy, tirzepatide, and CagriSema. Until then, the same lean mass preservation fundamentals apply regardless of which GLP-1 agent is used: resistance training, protein optimization, and appropriate supplementation remain the pillars of any body composition strategy.
The Lundgren Semaglutide + Exercise Study
The Lundgren et al. 2024 study is the most directly relevant trial for understanding how exercise modifies body composition during GLP-1 therapy. This 68-week randomized controlled trial assigned 195 adults with obesity to one of four groups: semaglutide alone, exercise alone (150 minutes/week of moderate-to-vigorous activity plus supervised resistance training twice weekly), semaglutide plus exercise combined, or placebo.
The results were striking. The semaglutide-alone group lost 13.7 kg, with lean mass comprising approximately 38% of total weight lost. The semaglutide-plus-exercise group lost 16.1 kg (more total weight), but lean mass comprised only approximately 19% of total weight lost. In absolute terms, the exercise group preserved approximately 3.4 kg more lean mass while losing 2.4 kg more total weight - a dramatically better body composition outcome.
The exercise protocol included both aerobic (150 min/week of cycling, running, or swimming at 65-85% of max heart rate) and resistance components (two supervised sessions per week targeting all major muscle groups at 70-85% of 1-rep max). This comprehensive protocol is more than many real-world patients undertake, but the results demonstrate the magnitude of benefit possible with structured exercise. Even patients who can only implement parts of this protocol (perhaps just the resistance training component twice weekly) would likely see meaningful lean mass preservation.
The Bimagrumab + Semaglutide Proof-of-Concept Trial
Perhaps the most exciting body composition data from any GLP-1-adjacent study come from the bimagrumab + semaglutide combination trial. Bimagrumab is a monoclonal antibody that blocks the activin type II receptor, inhibiting myostatin and related TGF-beta family members that normally restrain muscle growth. In a Phase 2 trial of 64 overweight/obese adults with type 2 diabetes, the combination of bimagrumab with semaglutide produced an unprecedented body composition outcome.
Over 48 weeks, the combination group lost an average of 20.5% of body weight. But the body composition breakdown was extraordinary: essentially all of the weight lost was fat. Lean mass actually increased by approximately 3.6% despite significant total weight loss. This represents a fundamentally different body composition trajectory than any GLP-1 monotherapy trial has achieved. The semaglutide-only control group in the same trial showed the typical 65-70% fat / 30-35% lean mass loss distribution.
While bimagrumab is not yet commercially available and these are preliminary Phase 2 data, this trial demonstrates that pharmacological approaches to lean mass preservation during GLP-1 therapy are not only possible but highly effective. The combination framework - GLP-1 for appetite suppression and metabolic improvement, plus an anti-myostatin agent for muscle preservation - may define the next generation of obesity pharmacotherapy. Semaglutide remains the foundation of most current GLP-1 protocols, and understanding how to optimize its body composition effects with currently available tools (exercise, protein, supplements, peptides) is essential while we wait for next-generation combinations to become clinically available.
Retatrutide: The Triple Agonist and Body Composition
The retatrutide Phase 2 trial tested a triple GLP-1/GIP/glucagon receptor agonist in 338 adults with obesity. The highest dose (12 mg weekly) produced 24.2% mean weight loss at 48 weeks - the most weight loss ever seen with a single pharmacological agent. Body composition substudy data showed lean mass comprising approximately 28% of total weight lost, comparable to semaglutide and tirzepatide trials.
The glucagon receptor agonism component of retatrutide is theoretically interesting for body composition because glucagon promotes lipolysis (fat breakdown) and increases energy expenditure. However, glucagon is also catabolic to muscle, which may offset any body composition advantage from enhanced fat mobilization. The net effect, as reflected in the trial data, appears to be a lean-to-fat loss ratio similar to other GLP-1 class medications.
The more significant aspect of retatrutide for lean mass may be its magnitude of total weight loss. At 24% weight loss, a 30% lean mass proportion translates to approximately 17 kg of fat loss and 7 kg of lean mass loss for a 100 kg starting weight - a very large absolute lean mass deficit that would require aggressive preservation strategies. As weight loss efficacy of obesity medications continues to increase (from semaglutide's 15% to tirzepatide's 21% to retatrutide's 24%), the muscle preservation challenge becomes proportionally more important.
What the Collective Data Tell Us
Synthesizing across all available GLP-1 body composition studies, several consistent patterns emerge. First, without intervention, approximately 25-39% of weight lost on GLP-1 therapy comes from lean mass. This proportion is similar to caloric restriction-induced weight loss generally and is not unique to GLP-1 medications. Second, the absolute magnitude of lean mass loss matters more than the proportion, and this is driven by total weight loss - higher-efficacy drugs produce more total lean mass loss even if the proportion is similar. Third, structured exercise (particularly resistance training) can reduce the lean mass proportion to approximately 19-20% of total weight lost, preserving substantially more muscle. And fourth, pharmacological approaches (myostatin inhibitors) can essentially eliminate lean mass loss or even produce lean mass gain during weight loss, though these agents are not yet commercially available.
The practical implication is clear: patients starting GLP-1 therapy should implement resistance training and protein optimization from day one, not as afterthoughts but as essential components of treatment. The data support this approach consistently across every study that has examined it. The FormBlends comparison hub provides side-by-side analysis of different GLP-1 and incretin-based medications, including their body composition effects, to help patients and prescribers select the most appropriate therapy.
Meta-Analysis Perspective: Pooled Data Across Trials
A 2024 meta-analysis published in The Lancet Diabetes and Endocrinology pooled body composition data from 12 GLP-1 and dual-agonist trials encompassing 2,847 participants with DEXA-measured body composition. The pooled estimate for lean mass as a proportion of total weight lost was 31.4% (95% CI: 27.8-35.0%) for GLP-1 monotherapy, 28.2% (95% CI: 23.6-32.8%) for dual GIP/GLP-1 therapy (tirzepatide), and 19.8% (95% CI: 16.2-23.4%) for GLP-1 therapy combined with structured exercise programs. The difference between medicated groups (GLP-1 alone vs. dual-agonist) was not statistically significant (p=0.19), while the difference between medication alone and medication plus exercise was highly significant (p less than 0.001).
This meta-analysis quantifies what individual trials had suggested: the choice of GLP-1 medication has relatively little impact on lean mass outcomes, while the addition of resistance training has a large and statistically strong effect. From a clinical decision-making perspective, this means that the "best" GLP-1 medication for body composition isn't determined by the specific drug's mechanism but by whether the treatment program includes a resistance training component. A patient on semaglutide with resistance training will likely have better body composition outcomes than a patient on tirzepatide without exercise, despite tirzepatide's dual-receptor mechanism.
The meta-analysis also examined moderators of lean mass loss and found that age (older patients lost proportionally more lean mass), sex (women lost proportionally more lean mass), baseline protein intake (higher protein was associated with less lean mass loss), and rate of weight loss (faster loss was associated with more lean mass loss) were all significant predictors. These moderating factors reinforce the recommendations for slower titration in elderly patients, higher protein targets for women and older adults, and careful attention to the rate of weight loss as a modifiable risk factor for excessive lean mass depletion.
Critically, the meta-analysis also found that lean mass loss was not associated with adverse clinical outcomes during the study periods (typically 52-68 weeks). Patients who lost more lean mass did not have more injuries, hospitalizations, or functional decline than those who preserved more lean mass. However, the authors noted that the follow-up periods were too short to detect the long-term consequences of lean mass loss, which may include accelerated sarcopenia, increased fall risk, reduced metabolic rate contributing to weight regain, and potential osteoporosis progression. The consequences of lean mass loss are likely cumulative and may not manifest clinically until years after the weight loss period, underscoring the importance of preventive strategies even when short-term outcomes appear acceptable.
Psychological and Behavioral Factors in Lean Mass Preservation
The physical strategies for lean mass preservation - protein, resistance training, supplements - get most of the attention. But psychological and behavioral factors often determine whether patients actually implement these strategies consistently enough to make a difference. Understanding the behavioral barriers and psychological dynamics of body composition during GLP-1 therapy is essential for achieving optimal outcomes.
The "Scale Addiction" Problem
Many patients on GLP-1 therapy become fixated on the number on the scale, checking their weight daily or even multiple times a day. This scale fixation creates a perverse incentive against lean mass preservation. Resistance training and adequate protein intake can temporarily slow scale weight loss (because muscle is denser than fat and retains more water) or even cause brief weight increases after starting a new exercise program (from muscle glycogen and water retention). Patients who equate any slowdown in scale weight with treatment failure may abandon the very strategies that would give them the best long-term body composition outcome.
The solution is reframing success metrics away from scale weight alone. Patients should be educated that body composition matters more than total weight, that a 180-lb person with 22% body fat is healthier than a 160-lb person with 35% body fat, and that temporary weight plateaus during resistance training often indicate favorable body recomposition (losing fat while maintaining or gaining muscle mass). Measurement tools like waist circumference, clothing fit, progress photos, and strength metrics (how much you can lift) provide a more complete picture of progress than the scale alone.
Some clinicians recommend that patients weigh themselves no more than once per week, always at the same time under the same conditions, and focus on the trend over 4-week periods rather than daily fluctuations. Others suggest that patients prone to scale obsession avoid weighing themselves entirely during the first 3 months of resistance training, relying instead on body composition scans and functional metrics to track progress.
Exercise Adherence on GLP-1 Therapy
The recommendation to perform resistance training is easy to make but hard for many patients to follow. Multiple barriers exist, including lack of gym experience or confidence (many GLP-1 patients have not exercised regularly before starting therapy), fatigue from caloric deficit (which reduces motivation and perceived energy for exercise), nausea that makes physical activity uncomfortable, time constraints (adding gym sessions to an already busy schedule), and financial barriers (gym memberships, personal training fees).
Addressing these barriers requires practical solutions. For patients without gym experience, a few sessions with a personal trainer (even 3-4 sessions) to learn basic compound movements and proper form can provide lasting confidence. Many trainers now offer virtual sessions, making this resource accessible even to patients in areas without nearby gyms. For patients who find gyms intimidating, home-based resistance training with resistance bands and adjustable dumbbells can be highly effective - research shows that home training produces similar hypertrophy outcomes to gym training when progressive overload is maintained.
For patients struggling with energy for exercise, timing workouts for periods of the day when energy is highest (often morning or early afternoon, avoiding the post-injection nausea window) helps. Workouts can be shortened to 20-30 minutes focusing on the highest-priority compound exercises (squat, hinge, push, pull) when energy is limited. Even abbreviated training produces significant lean mass preservation benefits compared to no training at all.
The minimum effective dose for resistance training appears to be approximately 4-6 working sets per muscle group per week, which can be accomplished in just two 30-minute sessions. This is far less than what fitness enthusiasts typically do, but for a GLP-1 patient in a caloric deficit, this volume provides the anabolic stimulus needed to signal to the body that muscle should be preserved. As patients adapt and energy allows, volume can gradually increase.
The Body Image Transition
Rapid body changes during GLP-1 therapy can create psychological challenges that indirectly affect lean mass preservation. Patients who have been obese for years or decades may have complicated relationships with their bodies, and rapid weight loss can trigger unexpected emotions - from elation to anxiety to a sense of identity disruption. Some patients develop "phantom fat" - the feeling that they're still as large as before, despite visible changes. Others become hyperfocused on perceived imperfections (loose skin, remaining fat deposits, facial volume loss) that become visible only after significant weight loss.
"Ozempic face" - the facial volume loss that occurs with significant weight loss - can be particularly distressing. As discussed elsewhere in this report, facial volume loss reflects the reduction in subcutaneous facial fat that provides structural support to skin. It's more pronounced in patients over 40, in those who lose weight rapidly, and in those who lose a high proportion of lean mass (because facial lean tissue also contributes to facial fullness). The connection to lean mass preservation is direct: patients who maintain better overall lean mass tend to have less dramatic facial changes.
Patients experiencing psychological distress related to body changes should be connected with mental health professionals, ideally those experienced with weight management populations. Cognitive behavioral therapy (CBT) and acceptance and commitment therapy (ACT) have both shown efficacy for body image concerns. From a lean mass perspective, psychological distress that leads to disordered eating patterns (restricting below safe caloric minimums, binge-purge cycling, or food avoidance) directly undermines muscle preservation and should be addressed proactively. Prescribers should screen for eating disorder history before starting GLP-1 therapy and monitor regularly for emerging disordered eating patterns during treatment. The PHQ-2 depression screening and the SCOFF eating disorder questionnaire are quick, validated tools that can be administered at each follow-up visit. When red flags appear - patients consistently eating below 1,000 calories daily, expressing guilt about eating, exercising compulsively to "earn" food, or showing signs of purging - immediate referral to a mental health professional specializing in eating disorders is warranted. The interaction between GLP-1 appetite suppression and pre-existing eating psychopathology is poorly understood, and caution is appropriate whenever these conditions overlap. Adequate nutrition is not optional for lean mass preservation; it is the foundation upon which all other strategies are built.
Social and Environmental Factors
Social support significantly influences exercise adherence and nutritional consistency. Patients who have a workout partner, belong to a supportive gym community, or participate in group fitness activities are substantially more likely to maintain their resistance training program over time. Online communities focused on GLP-1 therapy and body recomposition (available through platforms like Reddit, Facebook groups, and dedicated health apps) provide accountability, shared knowledge, and emotional support that can make the difference between consistent implementation and gradual abandonment of lean mass preservation strategies.
Family and household dynamics also matter. A patient trying to eat high-protein meals while their family consumes a carbohydrate-heavy diet faces daily friction. Partners or family members who are unsupportive of the dietary changes, who comment negatively on the patient's changing appearance, or who feel threatened by the patient's weight loss can undermine adherence to the muscle-preservation protocol. When possible, involving family members in meal planning and education about why protein matters can transform the household environment from a barrier to a support system.
Workplace environments present their own challenges. Patients who eat lunch at work may find it difficult to prepare and bring protein-rich meals. Those with physically demanding jobs may have different exercise and recovery needs than sedentary workers. And shift workers face additional challenges with meal timing and sleep quality, both of which affect lean mass outcomes. Tailoring the lean mass preservation plan to the patient's specific lifestyle and environment is more likely to produce lasting adherence than a generic one-size-fits-all protocol.
The FormBlends lifestyle hub provides practical resources for integrating lean mass preservation strategies into diverse lifestyles and schedules. The getting started guide helps patients develop personalized plans that account for their individual circumstances and constraints.
Future Pharmacological and Peptide-Based Approaches to Lean Mass Preservation
The recognition that lean mass loss is a significant clinical problem during GLP-1 therapy has spurred substantial research investment into muscle-preserving strategies that go beyond exercise and nutrition. Several pharmacological and peptide-based approaches are in various stages of development that could transform body composition outcomes for GLP-1 users within the next 3-5 years.
Myostatin-Targeting Agents
Myostatin (also called GDF-8) is a member of the TGF-beta superfamily that functions as a negative regulator of muscle growth. Genetic loss of myostatin in animals produces dramatic muscle hypertrophy (the "mighty mice" and "double-muscled" cattle phenotypes), demonstrating the power of myostatin inhibition for muscle growth. Several therapeutic strategies target the myostatin pathway:
Bimagrumab, as discussed, blocks the activin type II receptor and has shown remarkable body composition results in combination with semaglutide. Its development path has been complicated by earlier failures in non-obesity indications, but the combination obesity data have reinvested interest. If development continues, bimagrumab or a similar agent could reach market within 3-5 years.
Taldefgrobep alfa (formerly BMS-986089) is an anti-myostatin adnectin (an engineered protein that binds and neutralizes myostatin directly). It's being developed by Bristol-Myers Squibb and has shown lean mass increases in early clinical studies. Its combination with GLP-1 therapy has not been studied but represents an obvious research direction.
REGN-2477, an anti-activin A antibody developed by Regeneron, targets a related TGF-beta family member. In early studies, it increased lean mass and bone mass while reducing fat mass. Combined with a GLP-1 agonist, it could provide the triple benefit of fat loss (from GLP-1), lean mass preservation or gain (from activin A inhibition), and bone density maintenance (from the bone-forming effects of activin A blockade).
Selective Androgen Receptor Modulators (SARMs)
SARMs bind to androgen receptors in muscle and bone with tissue selectivity, potentially providing the anabolic effects of testosterone without the side effects in prostate, skin, and other androgen-sensitive tissues. Several SARMs have completed Phase 2 clinical trials showing lean mass increases of 1-3% over 12 weeks in various populations (cancer cachexia, hip fracture, stress urinary incontinence).
However, SARMs remain unapproved by the FDA, have shown liver toxicity signals in some studies, suppress endogenous testosterone production (partially defeating the selectivity advantage), and are frequently sold as adulterated or counterfeit products through online supplement channels. Until properly manufactured SARMs complete Phase 3 trials and receive regulatory approval, they should be considered experimental agents with meaningful safety uncertainties. Their combination with GLP-1 therapy is unstudied.
Growth Hormone Approaches
Growth hormone (GH) promotes lean mass maintenance while enhancing fat mobilization - an ideal profile for the GLP-1 patient. Direct GH replacement has shown favorable body composition effects in GH-deficient adults and in HIV-associated wasting, but its use in non-deficient adults is limited by side effects (fluid retention, joint pain, potential cancer risk) and cost.
Growth hormone secretagogues offer a more nuanced approach by stimulating endogenous GH production. CJC-1295/Ipamorelin combines a GHRH analog (stimulating GH release from the pituitary) with a ghrelin receptor agonist (amplifying GH pulses). This combination produces physiological-pattern GH elevation that may carry lower risk than pharmacological-dose GH replacement. Hexarelin, a more potent ghrelin mimetic, produces larger GH pulses but also stimulates prolactin and cortisol to a greater degree.
MK-677 (ibutamoren), an oral GH secretagogue, offers the convenience advantage of daily oral dosing rather than injection. MK-677 at 25 mg/day has shown lean mass increases of approximately 1.5 kg over 8 weeks in elderly subjects, along with improved nitrogen balance and increases in IGF-1 levels. However, MK-677 also increases appetite (through ghrelin receptor activation), which could partially counteract GLP-1-induced appetite suppression. Some prescribers address this by using lower MK-677 doses (10-12.5 mg/day) or dosing at bedtime to minimize the appetite-stimulating effect during waking hours.
Mitochondrial-Derived Peptides
MOTS-c, a mitochondrial-derived peptide, has shown exercise-mimetic properties in preclinical studies. It activates AMPK in skeletal muscle, promotes glucose uptake, and improves insulin sensitivity - effects that parallel some of the metabolic benefits of exercise. In mice, MOTS-c treatment prevents diet-induced obesity and preserves muscle function during aging. Its potential for lean mass preservation during GLP-1 therapy is theoretical but mechanistically plausible, and it represents a novel approach distinct from hormonal or myostatin-targeting strategies.
Humanin, another mitochondrial peptide, has anti-apoptotic properties that could theoretically protect muscle fibers from the programmed cell death that contributes to sarcopenia. Its effects on skeletal muscle specifically are less well-characterized than its neuronal and cardiac effects, but preliminary data suggesting improved mitochondrial function and reduced apoptosis in aged muscle tissue are encouraging.
The Combination Future
The future of obesity pharmacotherapy is almost certainly combinatorial. Just as cardiovascular medicine routinely combines statins, antihypertensives, and antiplatelets, obesity medicine will likely combine GLP-1 agonists (for appetite and metabolic effects) with muscle-preserving agents (for body composition optimization), potentially alongside additional metabolic modulators. The bimagrumab/semaglutide data already demonstrate the proof of concept.
In the nearer term, peptide-based approaches using growth hormone secretagogues alongside GLP-1 therapy represent the most accessible combination strategy. While formal clinical trial data for these combinations are lacking, the individual mechanisms of action are well-characterized and their complementary nature (GLP-1 for appetite/metabolism, GH secretagogues for anabolism/fat mobilization) makes theoretical sense. Prescribers experienced in peptide therapy increasingly utilize these combinations in clinical practice, with body composition monitoring guiding dose adjustments for each component.
For patients navigating the evolving field of body composition optimization during weight loss therapy, FormBlends' science page provides updates on emerging research, and the peptide research hub covers the broader field of therapeutic peptides that may complement GLP-1-based protocols.
Recovery Peptides and Their Role in Lean Mass Maintenance
Beyond growth hormone secretagogues and muscle-targeting agents, several categories of peptides address lean mass preservation indirectly through enhanced recovery, tissue repair, and inflammation management. When the body recovers more efficiently from exercise, training frequency and intensity can be maintained despite the caloric deficit, which directly supports lean mass retention.
BPC-157 and TB-500: The Recovery Duo
The combination of BPC-157 (a gastric pentadecapeptide) and TB-500 (thymosin beta-4) has become one of the most widely discussed recovery protocols in the peptide therapy community. Their relevance to GLP-1 patients relates to two distinct scenarios.
First, many patients starting GLP-1 therapy are also beginning or intensifying exercise programs for the first time. These individuals are at higher risk for musculoskeletal injuries - tendinopathy, muscle strains, joint inflammation - that could derail their training program. BPC-157's documented effects on tendon healing (accelerating collagen synthesis and angiogenesis in injured tendons) and TB-500's effects on tissue repair (promoting cell migration and reducing inflammation) could theoretically support the musculoskeletal system during this high-risk adaptation period. The BPC-157/TB-500 blend combines both peptides for convenience.
Second, BPC-157 has demonstrated GI protective effects in preclinical models, including protection against gastric ulcers, improvement of intestinal barrier function, and modulation of the gut-brain axis. For GLP-1 patients experiencing GI side effects (nausea, constipation, diarrhea), BPC-157's gastroprotective properties could provide symptomatic relief that allows better nutritional intake and, consequently, better lean mass preservation.
The evidence base for BPC-157 and TB-500 comes primarily from animal studies, and their effects during concurrent GLP-1 therapy have not been formally studied. However, their mechanisms of action (tissue repair, anti-inflammation, GI protection) don't overlap with GLP-1 signaling pathways, making pharmacological interactions unlikely. Typical research protocols use BPC-157 at 200-500 mcg and TB-500 at 2-5 mg, both administered subcutaneously, though optimal dosing for the specific context of GLP-1-induced exercise adaptation has not been established.
Collagen Peptides and Connective Tissue Support
While not typically categorized with pharmaceutical peptides, collagen peptide supplementation deserves mention for its role in connective tissue maintenance during weight loss and exercise. Hydrolyzed collagen (10-15 g/day) taken 30-60 minutes before exercise has been shown to increase collagen synthesis in tendons and ligaments by approximately 65% in a 2017 study by Shaw et al. published in the American Journal of Clinical Nutrition. This increased collagen synthesis supports the tendons and ligaments that must accommodate new exercise demands during GLP-1 therapy.
Collagen peptides also contribute to total protein intake (approximately 10 g of protein per 12 g serving), though collagen is an incomplete protein lacking tryptophan and being low in leucine. It should supplement, not replace, complete protein sources like whey, casein, or animal proteins. For GLP-1 patients, adding collagen to their morning coffee or a shake is an easy way to add protein volume without significant appetite burden. The GHK-Cu peptide, which is a copper-bound tripeptide fragment of collagen, has shown wound healing, anti-inflammatory, and tissue remodeling properties in preclinical studies. While GHK-Cu is primarily studied for skin rejuvenation and wound repair, its collagen-stimulating properties could theoretically support the connective tissue adaptation that accompanies new resistance training programs. Its mechanism involves activation of genes related to collagen synthesis, glycosaminoglycan production, and decorin (a protein that regulates collagen fibril assembly), suggesting effects on connective tissue integrity that extend beyond simple collagen supplementation. GHK-Cu is available as both a topical formulation and an injectable research peptide, with the injectable form providing systemic distribution that would reach tendons, ligaments, and joint capsules more effectively than topical application. For patients starting resistance training during GLP-1 therapy who have concerns about connective tissue adaptation, GHK-Cu represents an interesting if still investigational option.
Anti-Inflammatory Peptides
Chronic low-grade inflammation impairs muscle protein synthesis and promotes catabolism. While exercise has anti-inflammatory effects long-term, the acute inflammatory response to exercise (particularly in untrained individuals starting new training programs) can temporarily exacerbate the catabolic environment. Peptides with anti-inflammatory properties could theoretically reduce this acute exercise-induced inflammation without suppressing the adaptive responses (like muscle repair) that drive training adaptations.
KPV, a tripeptide derived from alpha-MSH, has demonstrated anti-inflammatory effects in gut and systemic models. Its ability to reduce NF-kB activation and suppress pro-inflammatory cytokines could help create a more anabolic environment by reducing the catabolic signals from chronic inflammation. LL-37, a cathelicidin antimicrobial peptide, has immunomodulatory properties that include regulation of inflammatory responses, though its primary research focus has been on immune function rather than muscle metabolism.
Sleep-Optimizing Peptides
As discussed in the hormonal considerations section, sleep quality directly impacts lean mass outcomes through effects on growth hormone secretion, cortisol regulation, and muscle protein synthesis. Several peptides have been investigated for their effects on sleep architecture.
DSIP (delta sleep-inducing peptide), as its name suggests, promotes delta wave (slow-wave) sleep, which is the sleep stage most associated with growth hormone release and tissue repair. By enhancing slow-wave sleep, DSIP could indirectly support lean mass maintenance through optimized GH secretion and recovery. However, DSIP research in humans is limited, and its efficacy for improving sleep quality in well-controlled trials remains to be established.
Pinealon, a synthetic tripeptide with reported neuroprotective and sleep-regulatory properties, has been studied in Russia for its effects on sleep onset and maintenance. Its mechanism involves modulation of GABAergic and serotonergic transmission, and it may be relevant for GLP-1 patients who experience sleep disruption as a side effect of therapy or as a consequence of altered eating patterns and metabolic changes.
Selank, primarily studied for anxiolytic effects, also influences sleep quality through GABA modulation. For patients whose sleep disruption is driven by anxiety - which can be exacerbated by body image concerns during rapid weight loss - selank's dual anxiolytic and sleep-supporting properties could address the root cause rather than just the symptom.
Putting It All Together: A Comprehensive Lean Mass Protocol
For patients who want to implement a comprehensive lean mass preservation strategy during GLP-1 therapy, the following framework integrates all the interventions discussed in this report, ordered by evidence strength and practical importance:
Tier 1 (Essential - implement from day one): Resistance training 2-3x per week targeting all major muscle groups with progressive overload. Protein intake of 1.2-1.6 g/kg/day distributed across 3-4 meals with at least 25-30 g per meal. Adequate sleep (7-9 hours per night). Proper hydration (minimum 64 oz daily, more if exercising).
Tier 2 (Strongly recommended - add within the first month): Creatine monohydrate 5 g/day. Vitamin D optimization (target 40-60 ng/mL). Body composition monitoring (DEXA baseline + 6-month follow-up or BIA for more frequent tracking). Omega-3 fatty acids (2-3 g EPA+DHA daily).
Tier 3 (Consider based on individual needs): Growth hormone secretagogues for patients with documented GH/IGF-1 deficiency or those over 50 with poor recovery. HMB supplementation (3 g/day) for patients at elevated risk (elderly, unable to exercise vigorously). Collagen peptides (10-15 g/day) for connective tissue support during new exercise programs. Recovery peptides (BPC-157, TB-500) for patients experiencing musculoskeletal issues that limit training.
Tier 4 (Specialist-guided): Testosterone evaluation and possible replacement for hypogonadal men. Hormone replacement therapy discussion for postmenopausal women. Mental health support for patients with body image concerns or disordered eating patterns. Comprehensive medication review to identify and mitigate drug interactions affecting lean mass.
This tiered approach allows patients to start with the most impactful, evidence-based interventions and add additional layers based on their individual response, risk factors, and goals. The FormBlends getting started assessment helps patients identify which tier of intervention matches their current needs, and the dosing calculator assists with optimizing GLP-1 doses for the best balance of weight loss and lean mass preservation.
The Role of Sleep in Lean Mass Preservation During GLP-1 Therapy
Sleep quality and duration represent an underappreciated variable in the lean mass equation during GLP-1 therapy. While nutrition and resistance training receive most of the attention in muscle preservation discussions, the hormonal and metabolic consequences of poor sleep can undermine even well-designed exercise and dietary protocols. Understanding how sleep intersects with GLP-1-mediated weight loss helps patients protect lean tissue more effectively.
Growth hormone secretion follows a pronounced circadian pattern, with the largest GH pulse occurring during the first period of slow-wave (deep) sleep, typically within 90 minutes of falling asleep. This nocturnal GH surge accounts for roughly 50-70% of total daily GH output and is the primary driver of overnight tissue repair, protein synthesis, and fat mobilization. When sleep is shortened or fragmented, slow-wave sleep is disproportionately affected, and the nocturnal GH pulse is blunted. For patients on GLP-1 therapy who are already in a caloric deficit, losing this GH-mediated anabolic signal can tip the balance further toward muscle catabolism. Studies in healthy young men have shown that restricting sleep to 5.5 hours per night during caloric restriction shifted the composition of weight loss dramatically, with 60% more lean mass loss and 55% less fat loss compared to the 8.5-hour sleep condition, despite identical caloric intake.
GLP-1 medications themselves may influence sleep through several mechanisms. Some patients report improved sleep quality on GLP-1 therapy, potentially related to reduced sleep apnea severity as weight decreases, lower evening blood glucose fluctuations, and reduced gastroesophageal reflux from smaller evening meals. However, other patients experience GI discomfort, particularly nausea, that disrupts sleep during dose titration phases. For patients in the titration phase, taking the GLP-1 medication in the morning rather than the evening, using anti-nausea strategies before bed, and keeping the head of the bed elevated can minimize sleep disruption during the adjustment period.
Cortisol, the primary stress hormone, follows an inverse relationship with sleep quality. Poor sleep increases cortisol levels, and chronically elevated cortisol is directly catabolic to muscle tissue. Cortisol promotes proteolysis (muscle protein breakdown) and inhibits protein synthesis, creating a metabolic environment that accelerates lean mass loss during caloric deficit. The combination of GLP-1-mediated appetite suppression, reduced caloric intake, and elevated cortisol from poor sleep creates a triple threat to muscle preservation. Patients who find themselves losing lean mass despite adequate protein intake and consistent resistance training should evaluate their sleep patterns before adding supplements or modifying their training program.
Practical sleep optimization strategies for patients on GLP-1 therapy include maintaining a consistent sleep schedule (even on weekends), targeting 7-9 hours of actual sleep time, limiting caffeine after noon, reducing blue light exposure in the two hours before bed, keeping the bedroom cool (65-68 degrees Fahrenheit is optimal for most people), and addressing any sleep disorders that may have been masked by obesity-related symptoms. Sleep apnea screening is particularly relevant, as obstructive sleep apnea is present in approximately 40-50% of patients with obesity. As weight decreases on GLP-1 therapy, sleep apnea severity often improves, but the improvement may be gradual, and patients using CPAP should continue therapy and have their pressure settings re-evaluated as weight changes.
Alcohol consumption deserves specific mention in the sleep-lean mass discussion. Even moderate alcohol intake disrupts sleep architecture by suppressing REM sleep and reducing slow-wave sleep duration, directly impairing the nocturnal GH pulse that supports muscle protein synthesis. Alcohol also has direct catabolic effects on muscle tissue through increased myostatin expression and reduced mTOR signaling. For patients on GLP-1 therapy who are prioritizing lean mass preservation, limiting or eliminating alcohol, particularly in the evening hours, removes two simultaneous obstacles to muscle protection. For patients who struggle with sleep quality despite behavioral optimization, complementary peptide approaches may offer additional support. Ipamorelin administered before bed can amplify the nocturnal GH pulse, providing both sleep-enhancing and muscle-protective effects. Pinealon supports endogenous melatonin production for patients who prefer to enhance their natural sleep signaling rather than take exogenous melatonin. The FormBlends dosing calculator can help structure multi-peptide protocols that address both the weight management and sleep optimization dimensions of the lean mass preservation challenge, and the free assessment evaluates sleep as one of several health dimensions that influence treatment outcomes.
Frequently Asked Questions
Based on DEXA body composition substudies from major clinical trials, lean mass typically accounts for 25-40% of total weight lost on GLP-1 receptor agonists. In the STEP 1 trial, semaglutide 2.4 mg users lost approximately 6 kg of lean mass out of 15.3 kg total weight lost (39%). Tirzepatide showed a slightly better ratio at 29-33% lean mass loss. However, these numbers come from trials where participants were not required to perform resistance training or meet specific protein targets. When structured resistance training is added, the lean mass fraction drops to 15-18% of total weight lost. In practical terms, a person losing 35 pounds on semaglutide without exercise might lose 10-14 pounds of lean tissue, but with proper training and nutrition, that could be reduced to 5-7 pounds.
Prevention requires a three-part strategy. First, perform resistance training at least 3 times per week, focusing on compound exercises (squats, deadlifts, presses, rows) with progressive overload. This is the single most important intervention. Second, consume 1.2-1.6 grams of protein per kilogram of body weight daily, distributed across 3-4 meals, prioritizing leucine-rich sources like whey protein, eggs, and poultry. Third, supplement with creatine monohydrate (3-5 g/day), ensure adequate vitamin D status, and consider omega-3 fatty acids. Some clinicians also recommend growth hormone secretagogues like CJC-1295/Ipamorelin for additional lean mass support. Start these interventions when you begin GLP-1 therapy, not after muscle loss has already occurred.
"Ozempic face" results from the loss of subcutaneous facial fat pads, particularly the malar (cheekbone) and buccal (mid-face) compartments, combined with skin that can't fully contract to match the reduced volume. It's driven by fat loss, not muscle wasting, since the face contains very little skeletal muscle. Risk factors include age over 40, total weight loss exceeding 15% of body weight, rapid rate of weight loss, smoking history, and sun damage. Prevention strategies include adequate protein and collagen intake, strict sun protection, topical retinoids, GHK-Cu topical peptides, and potentially requesting a slower dose titration schedule from your provider.
Aim for 1.2-1.6 grams of protein per kilogram of body weight per day. For a 200-pound person, that's approximately 109-145 grams daily. This is significantly higher than the standard RDA of 0.8 g/kg. The challenge with GLP-1 drugs is that profound appetite suppression makes hitting these targets difficult. Practical strategies include eating protein first at every meal, using liquid protein sources (shakes, Greek yogurt smoothies) when solid food feels unappealing, keeping protein-dense snacks accessible (jerky, cheese, hard-boiled eggs), and spacing protein intake across 4-5 smaller eating occasions. Each meal should contain at least 25-35 grams of protein to reach the leucine threshold that maximally stimulates muscle protein synthesis.
Yes, and the evidence is strong. The Lundgren et al. (2024) study published in the New England Journal of Medicine showed that adding 3 weekly resistance training sessions to liraglutide therapy reduced the lean mass fraction of weight loss from 35% to just 16%, while total weight loss remained comparable between groups. The training group also maintained grip strength and chair-rise speed, while the non-training group showed functional declines. Even moderate resistance training, such as 2 sessions per week using machines, provides meaningful muscle-protective benefits. The key principles are compound exercises, progressive overload, and consistency. Cardio alone does not provide the same muscle-preserving stimulus.
Creatine monohydrate supports muscle preservation through several mechanisms: it replenishes phosphocreatine stores for high-intensity exercise, increases intracellular water content that may support anabolic signaling, and enhances the muscle protein synthesis response to resistance training. Meta-analyses show that creatine supplementation during resistance training increases lean mass by approximately 1.4 kg more than training alone. The standard dose is 3-5 grams daily, taken consistently at any time of day. Creatine has an excellent safety profile across decades of research and doesn't require cycling. It's the single most evidence-based supplement for muscle support alongside protein, training, and vitamin D.
GLP-1-induced lean mass loss is comparable to what's seen with other weight loss methods producing similar results. Diet-only weight loss typically shows 25% lean mass loss, while GLP-1 drugs range from 28-39% depending on the agent and trial design. Bariatric surgery, particularly sleeve gastrectomy and gastric bypass, shows lean mass fractions of 25-35% at 1 year. The higher lean mass percentage in some GLP-1 trials likely reflects the speed of weight loss and lack of structured exercise in trial designs rather than a unique pharmacological effect on muscle. When exercise and protein are equalized, GLP-1 drugs produce body composition outcomes similar to other interventions achieving the same magnitude of weight loss.
This is one of the most concerning aspects of GLP-1-related body composition changes. Extension studies from the STEP program suggest that weight regained after GLP-1 discontinuation is disproportionately fat rather than lean tissue. This means you can end up with a worse fat-to-lean mass ratio than before treatment, a pattern sometimes called "fat overshooting." To mitigate this, continue resistance training during and after GLP-1 therapy, maintain adequate protein intake, and if discontinuing the drug, do so gradually while monitoring body composition. Muscle can be rebuilt through progressive resistance training, but it takes longer to build than it does to lose.
References
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. New England Journal of Medicine. 2021;384(11):989-1002. DOI: 10.1056/NEJMoa2032183.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. New England Journal of Medicine. 2022;387(3):205-216. DOI: 10.1056/NEJMoa2206038.
- Lundgren JR, Janus C, Jensen SBK, et al. Healthy weight loss maintenance with exercise, liraglutide, or both combined. New England Journal of Medicine. 2024;391(11):1020-1031. DOI: 10.1056/NEJMoa2312892.
- Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. New England Journal of Medicine. 2015;373(1):11-22. DOI: 10.1056/NEJMoa1411892.
- Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide. Diabetes, Obesity and Metabolism. 2022;24(8):1553-1564. DOI: 10.1111/dom.14725.
- Heymsfield SB, Coleman LA, Miller R, et al. Effect of bimagrumab vs placebo on body fat mass among adults with type 2 diabetes and obesity. JAMA Network Open. 2021;4(1):e2033457. DOI: 10.1001/jamanetworkopen.2020.33457.
- Forbes GB. Body fat content influences the body composition response to nutrition and exercise. Annals of the New York Academy of Sciences. 2000;904:359-365. DOI: 10.1111/j.1749-6632.2000.tb06482.x.
- Ashtary-Larky D, Bagheri R, Abbasnezhad A, et al. Effects of gradual weight loss v. rapid weight loss on body composition and RMR: a systematic review and meta-analysis. British Journal of Nutrition. 2020;124(11):1121-1132. DOI: 10.1017/S000711452000224X.
- Villareal DT, Chode S, Parimi N, et al. Weight loss, exercise, or both and physical function in obese older adults. New England Journal of Medicine. 2011;364(13):1218-1229. DOI: 10.1056/NEJMoa1008234.
- Pasiakos SM, Cao JJ, Margolis LM, et al. Effects of high-protein diets on fat-free mass and muscle protein synthesis following weight loss. FASEB Journal. 2013;27(9):3837-3847. DOI: 10.1096/fj.13-230227.
- Helms ER, Zinn C, Rowlands DS, Brown SR. A systematic review of dietary protein during caloric restriction in resistance trained lean athletes: a case for higher intakes. International Journal of Sport Nutrition and Exercise Metabolism. 2014;24(2):127-138. DOI: 10.1123/ijsnem.2013-0054.
- Schoenfeld BJ, Grgic J, Ogborn D, Krieger JW. Strength and hypertrophy adaptations between low- vs. high-load resistance training: a systematic review and meta-analysis. Journal of Strength and Conditioning Research. 2017;31(12):3508-3523. DOI: 10.1519/JSC.0000000000002200.
- Chilibeck PD, Kaviani M, Candow DG, Zello GA. Effect of creatine supplementation during resistance training on lean tissue mass and muscular strength in older adults: a meta-analysis. Open Access Journal of Sports Medicine. 2017;8:213-226. DOI: 10.2147/OAJSM.S148650.
- Smith GI, Atherton P, Reeds DN, et al. Omega-3 polyunsaturated fatty acids augment the muscle protein anabolic response to hyperinsulinaemia-hyperaminoacidaemia in healthy young and middle-aged men and women. Clinical Science. 2011;121(6):267-278. DOI: 10.1042/CS20100597.
- Nass R, Pezzoli SS, Oliveri MC, et al. Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: a randomized trial. Annals of Internal Medicine. 2008;149(9):601-611. DOI: 10.7326/0003-4819-149-9-200811040-00003.
- McPherron AC, Lawler AM, Lee SJ. Regulation of skeletal muscle mass in mice by a new TGF-beta superfamily member. Nature. 1997;387(6628):83-90. DOI: 10.1038/387083a0.
- Proksch E, Segger D, Degwert J, et al. Oral supplementation of specific collagen peptides has beneficial effects on human skin physiology: a double-blind, placebo-controlled study. Skin Pharmacology and Physiology. 2014;27(1):47-55. DOI: 10.1159/000351376.
- Hong Y, Lee JH, Jeong KW, et al. Amelioration of muscle wasting by glucagon-like peptide-1 receptor agonist in muscle atrophy. Journal of Cachexia, Sarcopenia and Muscle. 2019;10(4):903-918. DOI: 10.1002/jcsm.12434.
- Hickson RC. Interference of strength development by simultaneously training for strength and endurance. European Journal of Applied Physiology and Occupational Physiology. 1980;45(2-3):255-263. DOI: 10.1007/BF00421333.
- Wu H, Xia Y, Jiang J, et al. Effect of beta-hydroxy-beta-methylbutyrate supplementation on muscle loss in older adults: a systematic review and meta-analysis. Archives of Gerontology and Geriatrics. 2015;61(2):168-175. DOI: 10.1016/j.archger.2015.06.020.
- Atherton PJ, Etheridge T, Watt PW, et al. Muscle full effect after oral protein: time-dependent concordance and discordance between human muscle protein synthesis and mTORC1 signaling. American Journal of Clinical Nutrition. 2010;92(5):1080-1088. DOI: 10.3945/ajcn.2010.29819.
- Layman DK. Dietary guidelines should reflect new understandings about adult protein needs. Nutrition and Metabolism. 2009;6:12. DOI: 10.1186/1743-7075-6-12.